
Oxybutynin Chloride (oxybutynin chloride 5 mg) Dailymed
Generic: oxybutynin chloride is used for the treatment of Urinary Bladder, Neurogenic Colitis, Ulcerative Intestinal Obstruction Megacolon, Toxic Myasthenia Gravis Ureteral Obstruction Urinary Incontinence Glaucoma, Angle-Closure Urinary Retention Gastroparesis Dysuria Glaucoma

IMPRINT: A 31
SHAPE: round
COLOR: purple
All Imprints
24 hr oxybutynin chloride 15 mg extended release oral tablet - a 33 round white
24 hr oxybutynin chloride 10 mg extended release oral tablet - a 32 round pink
24 hr oxybutynin chloride 5 mg extended release oral tablet - a 31 round purple

Go PRO for all pill images
1 Indications And Usage
Oxybutynin chloride extended-release tablets are a muscarinic antagonist indicated for the treatment of overactive bladder with symptoms of urge urinary incontinence, urgency, and frequency.
Oxybutynin chloride extended-release tablets are also indicated for the treatment of pediatric patients aged 6 years and older with symptoms of detrusor overactivity associated with a neurological condition (e.g., spina bifida).
- Oxybutynin chloride extended-release tablets are a muscarinic antagonist indicated for the treatment of overactive bladder with symptoms of urge urinary incontinence, urgency, and frequency.
(1) - Oxybutynin chloride extended-release tablets are also indicated for the treatment of pediatric patients aged 6 years and older with symptoms of detrusor overactivity associated with a neurological condition (e.g., spina bifida).
(1)
2 Dosage And Administration
Oxybutynin chloride extended-release tablets must be swallowed whole with the aid of liquids, and must not be chewed, divided, or crushed.
Oxybutynin chloride extended-release tablets may be administered with or without food.
Oxybutynin chloride extended-release tablets must be swallowed whole with the aid of liquids, and must not be chewed, divided, or crushed. Oxybutynin chloride extended-release tablets may be administered with or without food.(2)
- Adults: Start with 5 mg or 10 mg, once daily at approximately the same time every day. Dose should not exceed 30 mg per day.
(2.1) - Pediatric patients (6 years of age or older): Start with 5 mg, once daily at approximately the same time every day. Dose should not exceed 20 mg per day.
(2.2) 2.1 Adults
The recommended starting dose of oxybutynin chloride extended-release tablets is 5 or 10 mg once daily at approximately the same time each day. Dosage may be adjusted in 5-mg increments to achieve a balance of efficacy and tolerability (up to a maximum of 30 mg/day). In general, dosage adjustment may proceed at approximately weekly intervals.
2.2 Pediatric Patients Aged 6 Years of Age and Older
The recommended starting dose of oxybutynin chloride extended-release tablets is 5 mg once daily at approximately the same time each day. Dosage may be adjusted in 5-mg increments to achieve a balance of efficacy and tolerability (up to a maximum of 20 mg/day).
3 Dosage Forms And Strengths
Oxybutynin chloride extended-release tablets, USP are available as 5 mg, 10 mg and 15 mg tablets for oral use:
5 mg: Purple, round, biconvex, coated tablets debossed with “A31” on one side and plain on the other side.
10 mg: Pink, round, biconvex, coated tablets debossed with “A32” on one side and plain on the other side.
15 mg: White, round, biconvex, coated tablets debossed with “A33” on one side and plain on the other side.
Extended-release tablets 5 mg, 10 mg and 15 mg(3)
4 Contraindications
Oxybutynin chloride extended-release tablets are contraindicated in patients with urinary retention, gastric retention and other severe decreased gastrointestinal motility conditions, uncontrolled narrow-angle glaucoma.
Oxybutynin chloride extended-release tablets are also contraindicated in patients who have demonstrated hypersensitivity to the drug substance or other components of the product. There have been reports of hypersensitivity reactions, including anaphylaxis and angioedema.
- Urinary retention
(4) - Gastric retention
(4) - Uncontrolled narrow angle glaucoma
(4) - Known hypersensitivity to oxybutynin chloride extended-release tablets, oxybutynin or any component of oxybutynin chloride extended-release tablets.
(4)
5 Warnings And Precautions
- Angioedema: Angioedema has been reported with oxybutynin. If symptoms of angioedema occur, discontinue oxybutynin chloride extended-release tablets immediately and initiate appropriate therapy.
(5.1) - Central Nervous System (CNS) Effects: CNS effects have been reported with oxybutynin. If patient experiences anticholinergic CNS effects, consider dose adjustment or discontinuation of oxybutynin chloride extended-release tablets.
(5.2) - Use with caution due to aggravation of symptoms:
- Pre-existing dementia in patients treated with cholinesterase inhibitors
(5.2) ,- Parkinson’s disease
(5.2) ,- Myasthenia gravis
(5.3) , and- Decreased gastrointestinal motility in patients with autonomic neuropathy
(5.4) .- Urinary Retention: Use with caution in patients with clinically significant bladder outflow obstruction because of the risk of urinary retention.
(5.5) - Gastrointestinal Adverse Reactions: Use with caution in patients with gastrointestinal obstructive disorders or decreased intestinal motility due to risk of gastric retention. Use with caution in patients with gastroesophageal reflux or in patients concurrently taking drugs that can exacerbate esophagitis.
(5.6) 5.1 Angioedema
Angioedema of the face, lips, tongue and/or larynx has been reported with oxybutynin. In some cases, angioedema occurred after the first dose. Angioedema associated with upper airway swelling may be life-threatening. If involvement of the tongue, hypopharynx, or larynx occurs, oxybutynin should be promptly discontinued and appropriate therapy and/or measures necessary to ensure a patent airway should be promptly provided.
5.2 Central Nervous System Effects
Oxybutynin is associated with anticholinergic central nervous system (CNS) effects [see Adverse Reactions (6)]. A variety of CNS anticholinergic effects have been reported, including hallucinations, agitation, confusion and somnolence. Patients should be monitored for signs of anticholinergic CNS effects, particularly in the first few months after beginning treatment or increasing the dose. Advise patients not to drive or operate heavy machinery until they know how oxybutynin chloride extended-release tablets affect them. If a patient experiences anticholinergic CNS effects, dose reduction or drug discontinuation should be considered.
Oxybutynin chloride extended-release tablets should be used with caution in patients with preexisting dementia treated with cholinesterase inhibitors due to the risk of aggravation of symptoms.
Oxybutynin chloride extended-release tablets should be used with caution in patients with Parkinson’s disease due to the risk of aggravation of symptoms.
5.3 Worsening of Symptoms of Myasthenia Gravis
Oxybutynin chloride extended-release tablets should be used with caution in patients with myasthenia gravis due to the risk of aggravation of symptoms.
5.4 Worsening of Symptoms of Decreased Gastrointestinal Motility in Patients with Autonomic Neuropathy
Oxybutynin chloride extended-release tablets should be used with caution in patients with autonomic neuropathy due to the risk of aggravation of symptoms of decreased gastrointestinal motility.
5.5 Urinary Retention
Oxybutynin chloride extended-release tablets should be administered with caution to patients with clinically significant bladder outflow obstruction because of the risk of urinary retention [see Contraindications (4)].
5.6 Gastrointestinal Adverse Reactions
Oxybutynin chloride extended-release tablets should be administered with caution to patients with gastrointestinal obstructive disorders because of the risk of gastric retention [see Contraindications (4)].
Oxybutynin chloride extended-release tablets, like other anticholinergic drugs, may decrease gastrointestinal motility and should be used with caution in patients with conditions such as ulcerative colitis and intestinal atony.
Oxybutynin chloride extended-release tablets should be used with caution in patients who have gastroesophageal reflux and/or who are concurrently taking drugs (such as bisphosphonates) that can cause or exacerbate esophagitis.
As with any other nondeformable material, caution should be used when administering oxybutynin chloride extended-release tablets to patients with preexisting severe gastrointestinal narrowing (pathologic or iatrogenic). There have been rare reports of obstructive symptoms in patients with known strictures in association with the ingestion of other drugs in nondeformable controlled-release formulations.
6 Adverse Reactions
The most common (incidence ≥5%) adverse reactions were dry mouth, constipation, diarrhea, headache, somnolence, and dizziness.(6)
To report SUSPECTED ADVERSE REACTIONS, contact Amneal Pharmaceuticals at 1-877-835-5472 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, the adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
The safety and efficacy of oxybutynin chloride extended-release tablets (5 to 30 mg/day) was evaluated in 774 adult subjects who participated in five double-blind, controlled clinical trials. In four of the five studies, oxybutynin chloride immediate-release tablets (5 to 20 mg/day in 199 subjects) was an active comparator. Adverse reactions reported by ≥ 1% of subjects are shown in Table 1.
Table 1: Adverse Drug Reactions Reported by ≥ 1% of Oxybutynin Chloride Extended-Release Tablets-treated Adult Subjects in Five Double-blind, Controlled Clinical Trials of Oxybutynin Chloride Extended-Release Tablets
System/Organ Class Preferred Term
Oxybutynin Chloride Extended-Release Tablets 5 to 30 mg/day n = 774 %
Oxybutynin Chloride Immediate-Release Tablets1 5 to 20 mg/day n = 199 %
Psychiatric Disorders
Insomnia
3.0
5.5
Nervous System Disorders
Headache
7.5
8.0
Somnolence
5.6
14.1
Dizziness
5.0
16.6
Dysgeusia
1.6
1.5
Eye Disorders
Vision blurred
4.3
9.6
Dry eye
3.1
2.5
Respiratory, Thoracic and Mediastinal Disorders
Cough
1.9
3.0
Oropharyngeal pain
1.9
1.5
Dry throat
1.7
2.5
Nasal dryness
1.7
4.5
Gastrointestinal Disorders
Dry mouth
34.9
72.4
Constipation
8.7
15.1
Diarrhea
7.9
6.5
Dyspepsia
4.5
6.0
Nausea
4.5
11.6
Abdominal pain
1.6
2.0
Vomiting
1.3
1.5
Flatulence
1.2
2.5
Gastro-esophageal reflux disease
1.0
0.5
Skin and Subcutaneous Tissue Disorders
Dry skin
1.8
2.5
Pruritus
1.3
1.5
Renal and Urinary Disorders
Dysuria
1.9
2.0
Urinary hesitation
1.9
8.5
Urinary retention
1.2
3.0
General Disorders and Administration Site Conditions
Fatigue
2.6
3.0
Investigations
Residual urine volume2
2.3
3.5
1 IR = immediate-release
2 The bundled term residual urine volume consists of the preferred terms residual urine volume and residual urine volume increased.
The discontinuation rate due to adverse reactions was 4.4% with oxybutynin chloride extended-release tablets compared to 0% with oxybutynin chloride immediate-release tablets. The most frequent adverse reaction causing discontinuation of study medication was dry mouth (0.7%).
The following adverse reactions were reported by <1% of oxybutynin chloride extended-release tablets-treated patients and at a higher incidence than placebo in clinical trials: Metabolism and Nutrition Disorders: anorexia, fluid retention; Vascular disorders: hot flush; Respiratory, thoracic and mediastinal disorders: dysphonia; Gastrointestinal Disorders: dysphagia, frequent bowel movements; General disorders and administration site conditions: chest discomfort, thirst.
6.2 Postmarketing Experience
The following additional adverse reactions have been reported from worldwide postmarketing experience with oxybutynin chloride extended-release tablets. Because postmarketing reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Infections and Infestations: Urinary tract infection; Psychiatric Disorders: psychotic disorder, agitation, confusional state, hallucinations, memory impairment, abnormal behavior; Nervous System Disorders: convulsions; Eye Disorders: glaucoma; Respiratory, Thoracic and Mediastinal Disorders: nasal congestion; Cardiac Disorders: arrhythmia, tachycardia, palpitations, QT interval prolongation; Vascular Disorders: flushing, hypertension; Skin and Subcutaneous Tissue Disorders: rash; Renal and Urinary Disorders: impotence; General Disorders and Administration Site Conditions: hypersensitivity reactions, including angioedema with airway obstruction, urticaria, and face edema; anaphylactic reactions requiring hospitalization for emergency treatment; Injury, poisoning and procedural complications: fall.
Additional adverse events reported with some other oxybutynin chloride formulations include: cycloplegia, mydriasis, and suppression of lactation. In one reported case, concomitant use of oxybutynin with carbamazepine and dantrolene was associated with adverse events of vomiting, drowsiness, confusion, unsteadiness, slurred speech and nystagmus, suggestive of carbamazepine toxicity.
7 Drug Interactions
The concomitant use of oxybutynin with other anticholinergic drugs or with other agents which produce dry mouth, constipation, somnolence (drowsiness), and/or other anticholinergic-like effects may increase the frequency and/or severity of such effects.
Anticholinergic agents may potentially alter the absorption of some concomitantly administered drugs due to anticholinergic effects on gastrointestinal motility. This may be of concern for drugs with a narrow therapeutic index. Anticholinergic agents may also antagonize the effects of prokinetic agents, such as metoclopramide.
Mean oxybutynin plasma concentrations were approximately 2 fold higher when oxybutynin chloride extended-release tablets was administered with ketoconazole, a potent CYP3A4 inhibitor. Other inhibitors of the cytochrome P450 3A4 enzyme system, such as antimycotic agents (e.g., itraconazole and miconazole) or macrolide antibiotics (e.g., erythromycin and clarithromycin), may alter oxybutynin mean pharmacokinetic parameters (i.e., Cmax and AUC). The clinical relevance of such potential interactions is not known. Caution should be used when such drugs are co-administered.
- Co-administration with other anticholinergic drugs may increase the frequency and/or severity of anticholinergic-like effects.
(7) - Co-administration with strong cytochrome P450 (CYP) 3A4 inhibitors (e.g., ketoconazole) increases the systemic exposure of oxybutynin.
(7)
8 Use In Specific Populations
- Pediatric Use: Oxybutynin chloride extended-release tablets are not recommended in pediatric patients who cannot swallow the tablet whole without chewing, dividing or crushing, or in children under the age of 6 years.
(8.4) - Renal or Hepatic Impairment: There have been no studies conducted in patients with renal or hepatic impairment.
(8.6, 8.7) 8.1 Pregnancy
Risk Summary
There are no adequate data on oxybutynin chloride extended-release tablets use in pregnant women to evaluate for a drug-associated risk of major birth defects, miscarriage or adverse maternal or fetal outcomes.
In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively. The background risk of major birth defects and miscarriage for the indicated population is unknown.
8.2Lactation
Risk Summary
There are no data on the presence of oxybutynin in human milk, the effects on the breastfed infant, or the effects of oxybutynin chlorideextended-release tablets on milk production. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for oxybutynin chlorideextended-release tablets and any potential adverse effects on the breastfed child from oxybutynin chlorideextended-release tablets or from the underlying maternal condition.
8.4 Pediatric Use
The safety and efficacy of oxybutynin chloride extended-release tablets were studied in 60 children in a 24-week, open-label, non-randomized trial. Patients were aged 6 to 15 years, all had symptoms of detrusor overactivity in association with a neurological condition (e.g., spina bifida), all used clean intermittent catheterization, and all were current users of oxybutynin chloride. Study results demonstrated that administration of oxybutynin chloride extended-release tablets 5 to 20 mg/day was associated with an increase from baseline in mean urine volume per catheterization from 108 mL to 136 mL, an increase from baseline in mean urine volume after morning awakening from 148 mL to 189 mL, and an increase from baseline in the mean percentage of catheterizations without a leaking episode from 34% to 51%.
Urodynamic results were consistent with clinical results. Administration of oxybutynin chloride extended-release tablets resulted in an increase from baseline in mean maximum cystometric capacity from 185 mL to 254 mL, a decrease from baseline in mean detrusor pressure at maximum cystometric capacity from 44 cm H2O to 33 cm H2O, and a reduction in the percentage of patients demonstrating uninhibited detrusor contractions (of at least 15 cm H2O) from 60% to 28%.
The pharmacokinetics of oxybutynin chloride extended-release tablets in these patients were consistent with those reported for adults [see Clinical Pharmacology (12.3)].
Oxybutynin chloride extended-release tablets are not recommended in pediatric patients who cannot swallow the tablet whole without chewing, dividing, or crushing, or in children under the age of 6.
8.5 Geriatric Use
The rate and severity of anticholinergic effects reported by patients less than 65 years old and those 65 years and older were similar. The pharmacokinetics of oxybutynin chloride extended-release tablets were similar in all patients studied (up to 78 years of age).
8.6 Renal Impairment
There were no studies conducted with oxybutynin chloride extended-release tablets in patients with renal impairment.
8.7 Hepatic Impairment
There were no studies conducted with oxybutynin chloride extended-release tablets in patients with hepatic impairment.
10 Overdosage
The continuous release of oxybutynin from oxybutynin chloride extended-release tablets should be considered in the treatment of overdosage. Patients should be monitored for at least 24 hours. Treatment should be symptomatic and supportive. A cathartic may be administered.
Overdosage with oxybutynin chloride has been associated with anticholinergic effects including central nervous system excitation, flushing, fever, dehydration, cardiac arrhythmia, vomiting, and urinary retention.
Ingestion of 100 mg oxybutynin chloride in association with alcohol has been reported in a 13-year-old boy who experienced memory loss, and a 34-year-old woman who developed stupor, followed by disorientation and agitation on awakening, dilated pupils, dry skin, cardiac arrhythmia, and retention of urine. Both patients fully recovered with symptomatic treatment.
11 Description
Oxybutynin chloride, USP is an antispasmodic, muscarinic antagonist. Each oxybutynin chloride extended-release tablet, USP contains 5 mg, 10 mg, or 15 mg of oxybutynin chloride USP, formulated as a once-a-day controlled-release tablet for oral administration. Oxybutynin chloride, USP is administered as a racemate of R- and S-enantiomers.
Chemically, oxybutynin chloride, USP is d,l (racemic) 4-diethylamino-2-butynyl phenylcyclohexylglycolate hydrochloride. The empirical formula of oxybutynin chloride, USP is C22H31NO3•HCl.
Its structural formula is:
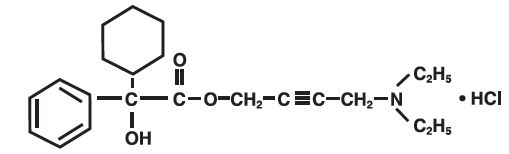
Oxybutynin chloride, USP is a white crystalline solid with a molecular weight of 393.9. It is readily soluble in water and acids, but relatively insoluble in alkalis.
Oxybutynin chloride extended-release tablets, USP also contains the following inert ingredients: hydrogenated vegetable oil, hypromellose, isopropyl alcohol, lactose monohydrate, methacrylic acid copolymer, microcrystalline cellulose, polysorbate 80, sodium lauryl sulfate, talc and triethyl citrate. The 5 mg tablets also contain D&C Red #27 and FD&C Blue #1. The 10 mg tablets also contain FD&C Red #40 and FD&C Yellow #6.
Meets USP Dissolution Test 7.
System Components and Performance
Oxybutynin chloride extended-release tablet, USP uses a pH-independent hydrophilic matrix and pH dependent enteric coating to deliver oxybutynin chloride, USP at a controlled rate over approximately 24 hours. The oxybutynin chloride extended-release tablet, USP comprises of an inner core made of the drug, rate controlling pH independent polymer and other excipients. The tablet core is then coated with pH dependent enteric coating polymer. When tablets will be exposed to an acidic environment such as the stomach, the drug release will be minimal due to outer enteric coating of the pH dependent polymer. The outer enteric coating upon reaching an environment of pH 5.5 and above will start to dissolve and the polymer in the inner core tablet will hydrate to form a gel layer and the drug releases via diffusion process.
12 Clinical Pharmacology
12.1 Mechanism of Action
Oxybutynin relaxes bladder smooth muscle. Oxybutynin chloride exerts a direct antispasmodic effect on smooth muscle and inhibits the muscarinic action of acetylcholine on smooth muscle. No blocking effects occur at skeletal neuromuscular junctions or autonomic ganglia (antinicotinic effects).
Antimuscarinic activity resides predominantly in the R-isomer. A metabolite, desethyloxybutynin, has pharmacological activity similar to that of oxybutynin in in vitro studies.
12.2 Pharmacodynamics
In patients with conditions characterized by involuntary bladder contractions, cystometric studies have demonstrated that oxybutynin increases bladder (vesical) capacity, diminishes the frequency of uninhibited contractions of the detrusor muscle, and delays the initial desire to void.
12.3 Pharmacokinetics
Absorption
Following the first dose of oxybutynin chloride extended-release tablets, oxybutynin plasma concentrations rise for 4 to 6 hours; thereafter steady concentrations are maintained for up to 24 hours, minimizing fluctuations between peak and trough concentrations associated with oxybutynin.
The relative bioavailabilities of R- and S-oxybutynin from oxybutynin chloride extended-release tablets are 156% and 187%, respectively, compared with oxybutynin. The mean pharmacokinetic parameters for R- and S-oxybutynin are summarized in Table 2. The plasma concentration-time profiles for R- and S-oxybutynin are similar in shape; Figure 1 shows the profile for R-oxybutynin.
Table 2: Mean (SD) R- and S-Oxybutynin Pharmacokinetic Parameters Following a Single Dose of Oxybutynin Chloride Extended-Release Tablets 10 mg (n=43)
Parameters (units)
R-Oxybutynin
S-Oxybutynin
Cmax (ng/mL)
1.0
(0.6)
1.8
(1.0)
Tmax (h)
12.7
(5.4)
11.8
(5.3)
t1/2 (h)
13.2
(6.2)
12.4
(6.1)
AUC(0-48) (ng•h/mL)
18.4
(10.3)
34.2
(16.9)
AUCinf (ng•h/mL)
21.3
(12.2)
39.5
(21.2)
Figure 1: Mean R-oxybutynin plasma concentrations following a single dose of oxybutynin chloride extended-release tablets 10 mg and oxybutynin 5 mg administered every 8 hours (n=23 for each treatment).
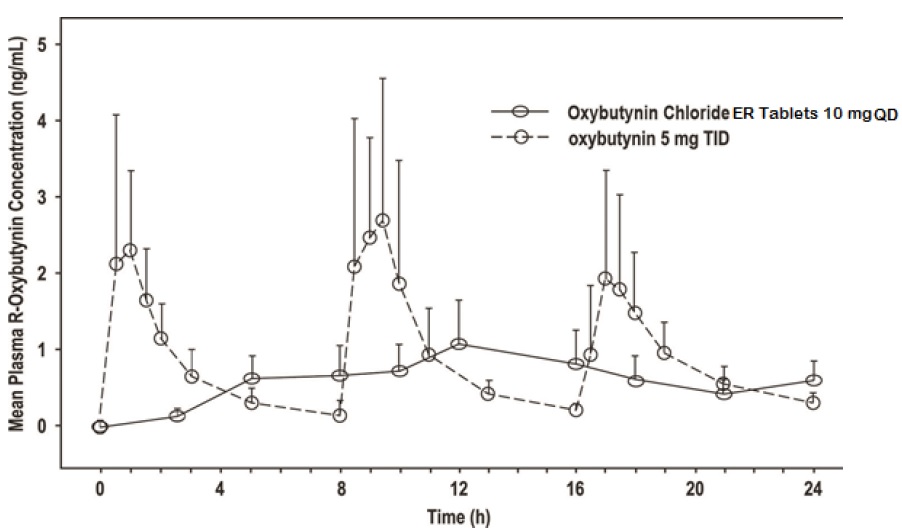
Steady-state oxybutynin plasma concentrations are achieved by Day 3 of repeated oxybutynin chloride extended-release tablets dosing, with no observed drug accumulation or change in oxybutynin and desethyloxybutynin pharmacokinetic parameters.
Oxybutynin chloride extended-release tablets steady-state pharmacokinetics were studied in 19 children aged 5 to 15 years with detrusor overactivity associated with a neurological condition (e.g., spina bifida). The children were on oxybutynin chloride extended-release tablets total daily dose ranging from 5 to 20 mg (0.10 to 0.77 mg/kg). Sparse sampling technique was used to obtain serum samples. When all available data are normalized to an equivalent of 5 mg per day of oxybutynin chloride extended-release tablets, the mean pharmacokinetic parameters derived for R- and S-oxybutynin and R- and S-desethyloxybutynin are summarized in Table 3. The plasma-time concentration profiles for R- and S-oxybutynin are similar in shape; Figure 2 shows the profile for R-oxybutynin when all available data are normalized to an equivalent of 5 mg per day.
Table 3: Mean ± SD R- and S-Oxybutynin and R- and S-Desethyloxybutynin Pharmacokinetic Parameters in Children Aged 5 to 15 Following Administration of 5 to 20 mg Oxybutynin Chloride Extended-Release Tablets Once Daily (n=19), All Available Data Normalized to an Equivalent of Oxybutynin Chloride Extended-Release Tablets 5 mg Once Daily
R-Oxybutynin
S-Oxybutynin
R-Desethyloxybutynin
S-Desethyloxybutynin
Cmax (ng/mL)
0.7 ± 0.4
1.3 ± 0.8
7.8 ± 3.7
4.2 ± 2.3
Tmax (h)
5.0
5.0
5.0
5.0
AUC (ng•h/mL)
12.8 ± 7.0
23.7 ± 14.4
125.1 ± 66.7
73.6 ± 47.7
Figure 2: Mean steady-state (± SD) R-oxybutynin plasma concentrations following administration of 5 to 20 mg Oxybutynin Chloride Extended-Release Tablets once daily in children aged 5 to 15. Plot represents all available data normalized to an equivalent of Oxybutynin Chloride Extended-Release Tablets 5 mg once daily.
Food Effects
The rate and extent of absorption and metabolism of oxybutynin are similar under fed and fasted conditions.
Distribution
Oxybutynin is widely distributed in body tissues following systemic absorption. The volume of distribution is 193 L after intravenous administration of 5 mg oxybutynin chloride. Both enantiomers of oxybutynin are highly bound (>99%) to plasma proteins. Both enantiomers of N-desethyloxybutynin are also highly bound (>97%) to plasma proteins. The major binding protein is alpha-1 acid glycoprotein.
Metabolism
Oxybutynin is metabolized primarily by the cytochrome P450 enzyme systems, particularly CYP3A4 found mostly in the liver and gut wall. Its metabolic products include phenylcyclohexylglycolic acid, which is pharmacologically inactive, and desethyloxybutynin, which is pharmacologically active. Following oxybutynin chloride extended-release tablets administration, plasma concentrations of R- and S-desethyloxybutynin are 73% and 92%, respectively, of concentrations observed with oxybutynin.
Excretion
Oxybutynin is extensively metabolized by the liver, with less than 0.1% of the administered dose excreted unchanged in the urine. Also, less than 0.1% of the administered dose is excreted as the metabolite desethyloxybutynin.
Dose Proportionality
Pharmacokinetic parameters of oxybutynin and desethyloxybutynin (Cmax and AUC) following administration of 5 mg to 20 mg of oxybutynin chloride extended-release tablets are dose proportional.
Use in Specific Populations
Pediatric
The pharmacokinetics of oxybutynin chloride extended-release tablets were evaluated in 19 children aged 5 to 15 years with detrusor overactivity associated with a neurological condition (e.g., spina bifida). The pharmacokinetics of oxybutynin chloride extended-release tablets in these pediatric patients were consistent with those reported for adults (see Tables 2 and 3, and Figures 1 and 2 above).
Gender
There are no significant differences in the pharmacokinetics of oxybutynin in healthy male and female volunteers following administration of oxybutynin chloride extended-release tablets.
Race
Available data suggest that there are no significant differences in the pharmacokinetics of oxybutynin based on race in healthy volunteers following administration of oxybutynin chloride extended-release tablets.
13 Nonclinical Toxicology
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
A 24-month study in rats at dosages of oxybutynin chloride of 20, 80, and 160 mg/kg/day showed no evidence of carcinogenicity. These doses are approximately 6, 25, and 50 times the maximum human exposure, based on a human equivalent dose taking into account normalization of body surface area.
Mutagenesis
Oxybutynin chloride showed no increase of mutagenic activity when tested in Schizosaccharomyces pompholiciformis, Saccharomyces cerevisiae, and Salmonella typhimurium test systems.
Impairment of Fertility
No impairment of fertility was seen in rats at dosages up to 75 mg/kg/day (24 times the MRHD on a mg/m2 basis) when administered for 2 weeks prior to mating in females and for 9 weeks prior to mating in males.
14 Clinical Studies
Oxybutynin chloride extended-release tablets was evaluated for the treatment of patients with overactive bladder with symptoms of urge urinary incontinence, urgency, and frequency in three controlled efficacy studies. The majority of patients were Caucasian (89.0%) and female (91.9%) with a mean age of 59 years (range, 18 to 98 years). Entry criteria required that patients have urge or mixed incontinence (with a predominance of urge) as evidenced by ≥ 6 urge incontinence episodes per week and ≥ 10 micturitions per day. Study 1 was a fixed-dose escalation design, whereas the other two studies used a dose-adjustment design in which each patient’s final dose was adjusted to a balance between improvement of incontinence symptoms and tolerability of side effects. All three studies included patients known to be responsive to oxybutynin or other anticholinergic medications, and these patients were maintained on a final dose for up to 2 weeks.
The efficacy results for the three controlled trials are presented in the following Tables 4, 5 and 6 and Figures 3, 4 and 5.
Table 4: Number of Urge Urinary Incontinence Episodes Per Week (Study 1)
Study 1
n
Oxybutynin Chloride Extended-Release Tablets
n
Placebo
Mean Baseline
34
15.9
16
20.9
Mean (SD) Change from Baseline†
34
-15.8 (8.9)
16
-7.6 (8.6)
95% Confidence Interval for Difference
(-13.6, -2.8)*
(Oxybutynin Chloride Extended-Release Tablets – Placebo)
* The difference between oxybutynin chloride extended-release tablets and placebo was statistically significant.
† Covariate adjusted mean with missing observations set to baseline values.
Figure 3: Mean Change (±SD) in Urge Urinary Incontinence Episodes Per Week from Baseline (Study 1)
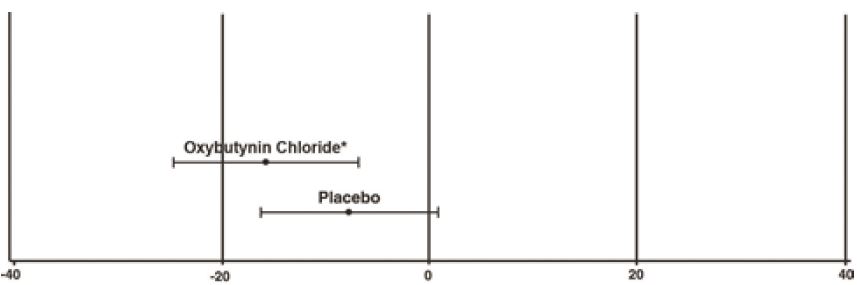
* The difference between oxybutynin chloride and placebo was statistically significant.
Table 5: Number of Urge Urinary Incontinence Episodes Per Week (Study 2)
Study 2
n
Oxybutynin Chloride Extended-Release Tablets
n
Oxybutynin
Mean Baseline
53
27.6
52
23
Mean (SD) Change from Baseline†
53
-17.6 (11.9)
52
-19.4 (11.9)
95% Confidence Interval for Difference
(-2.8, 6.5)
(Oxybutynin Chloride Extended-Release Tablets – Oxybutynin)
† Covariate adjusted mean with missing observations set to baseline values.
Figure 4: Mean Change (±SD) in Urge Urinary Incontinence Episodes Per Week from Baseline (Study 2)
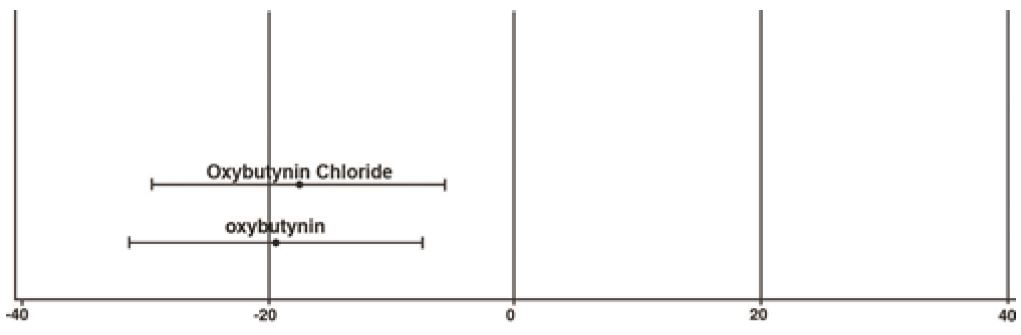
Table 6: Number of Urge Urinary Incontinence Episodes Per Week (Study 3)
Study 3
n
Oxybutynin Chloride Extended-Release Tablets
n
Oxybutynin
Mean Baseline
111
18.9
115
19.5
Mean (SD) Change from Baseline†
111
-14.5 (8.7)
115
-13.8 (8.6)
95% Confidence Interval for Difference
(-3, 1.6)**
(Oxybutynin Chloride Extended-Release Tablets – Oxybutynin)
** The difference between oxybutynin chloride extended-release tablets and oxybutynin fulfilled the criteria for comparable efficacy.
† Covariate adjusted mean with missing observations set to baseline values.
Figure 5: Mean Change (±SD) in Urge Urinary Incontinence Episodes Per Week from Baseline (Study 3)
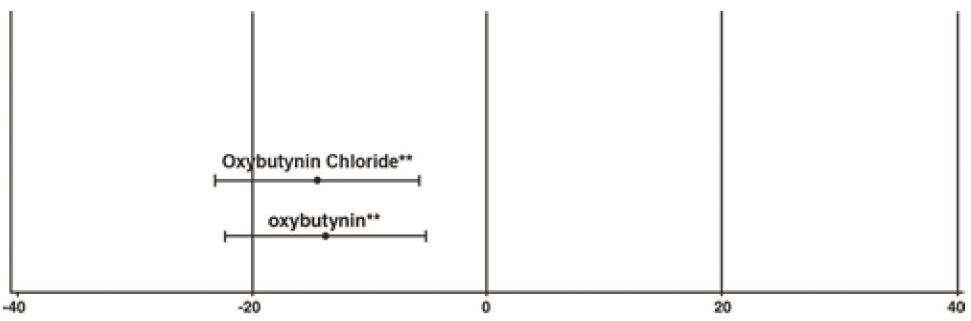
** The difference between oxybutynin chloride and oxybutynin fulfilled the criteria for comparable efficacy.
16 How Supplied/storage Andhandling
Oxybutynin chloride extended-release tablets USP, 5 mg are supplied as purple, round, biconvex, coated tablets debossed with “A31” on one side and plain on the other side. They are available as follows:
Bottles of 30: NDC 65162-371-03 Bottles of 90: NDC 65162-371-09 Bottles of 100: NDC 65162-371-10 Bottles of 500: NDC 65162-371-50
Oxybutynin chloride extended-release tablets USP, 10 mg are supplied as pink, round, biconvex, coated tablets debossed with “A32” on one side and plain on the other side. They are available as follows:
Bottles of 30: NDC 65162-372-03 Bottles of 90: NDC 65162-372-09 Bottles of 100: NDC 65162-372-10 Bottles of 500: NDC 65162-372-50
Oxybutynin chloride extended-release tablets USP, 15 mg are supplied as white, round, biconvex, coated tablets debossed with “A33” on one side and plain on the other side. They are available as follows:
Bottles of 30: NDC 65162-373-03 Bottles of 90: NDC 65162-373-09 Bottles of 100: NDC 65162-373-10 Bottles of 250: NDC 65162-373-25Bottles of 500: NDC 65162-373-50
Store at 20° to 25°C (68° to 77°F); excursions permitted between 15° to 30°C (59° to 86°F) [see USP Controlled Room Temperature]. Protect from moisture and humidity.
Keep out of the reach of children.
17 Patient Counseling Information
- Patients should be informed that oxybutynin may produce angioedema that could result in life threatening airway obstruction. Patients should be advised to promptly discontinue oxybutynin therapy and seek immediate medical attention if they experience swelling of the tongue, edema of the laryngopharynx, or difficulty breathing.
- Patients should be informed that anticholinergic (antimuscarinic) agents such as oxybutynin chloride extended-release tablets, may produce clinically significant adverse reactions related to anticholinergic activity such as:
- Urinary retention and constipation
- Heat prostration due to decreased sweating. Heat prostration can occur when anticholinergic medicines are administered in the presence of high environmental temperature.
- Patients should be informed that anticholinergic medicines such as oxybutynin chloride extended-release tablets may produce drowsiness (somnolence), dizziness or blurred vision. Patients should be advised to exercise caution in decisions to engage in potentially dangerous activities until oxybutynin chloride extended-release tablets effects have been determined.
- Patients should be informed that alcohol may enhance the drowsiness caused by anticholinergic agents such as oxybutynin chloride extended-release tablets.
- Patients should be informed that oxybutynin chloride extended-release tablets should be swallowed whole with the aid of liquids. Patients should not chew, divide, or crush tablets. The medication is contained within a nonabsorbable shell designed to release the drug at a controlled rate. The tablet shell is eliminated from the body; patients should not be concerned if they occasionally notice in their stool something that looks like a tablet.
- Oxybutynin chloride extended-release tablets should be taken at approximately the same time each day.
For more information call 1-877-835-5472 or visit www.amneal.com
* Trademarks are the property of their respective owners.
Distributed by: Amneal Pharmaceuticals LLC Bridgewater, NJ 08807
Rev. 02-2023-10
Principal Display Panel
DISCLAIMER:
"This tool does not provide medical advice, and is for informational and educational purposes only, and is not a substitute for professional medical advice, treatment or diagnosis. Call your doctor to receive medical advice. If you think you may have a medical emergency, please dial 911."
"Do not rely on openFDA to make decisions regarding medical care. While we make every effort to ensure that data is accurate, you should assume all results are unvalidated. We may limit or otherwise restrict your access to the API in line with our Terms of Service."
"This product uses publicly available data from the U.S. National Library of Medicine (NLM), National Institutes of Health, Department of Health and Human Services; NLM is not responsible for the product and does not endorse or recommend this or any other product."
PillSync may earn a commission via links on our site
