Methylphenidate Hydrochloride (methylphenidate hydrochloride 60 mg) Dailymed
Generic: methylphenidate hydrochloride is used for the treatment of Anxiety Disorders Attention Deficit Disorder with Hyperactivity Depressive Disorder Tourette Syndrome Glaucoma Narcolepsy Psychomotor Agitation Tics

IMPRINT: CP 402 20MG
SHAPE: capsule
COLOR: white
All Imprints
30/70 release 24 hr methylphenidate hydrochloride 40 mg extended release oral capsule - cp 404 40mg capsule white
30/70 release 24 hr methylphenidate hydrochloride 50 mg extended release oral capsule - cp 405 50mg capsule white
30/70 release 24 hr methylphenidate hydrochloride 20 mg extended release oral capsule - cp 402 20mg capsule white
30/70 release 24 hr methylphenidate hydrochloride 10 mg extended release oral capsule - cp 401 10mg capsule white
30/70 release 24 hr methylphenidate hydrochloride 60 mg extended release oral capsule - cp 406 60mg capsule white
30/70 release 24 hr methylphenidate hydrochloride 30 mg extended release oral capsule - cp 403 30mg capsule white
Boxed Warning
Warning: Abuse, Misuse, And Addiction
- Before prescribing methylphenidate hydrochloride extended-release , assess each patient’s risk for abuse, misuse, and addiction.
- Educate patients and their families about these risks, proper storage of the drug, and proper disposal of any unused drug.
- Throughout treatment, reassess each patient’s risk and frequently monitor for signs and symptoms of abuse, misuse, and addiction.

Go PRO for all pill images
Warning: Abuse, Misuse, And Addiction
Methylphenidate hydrochloride extended-release has a high potential for abuse and misuse, which can lead to the development of a substance use disorder, including addiction. Misuse and abuse of CNS stimulants, including methylphenidate hydrochloride extended-release, can result in overdose and death [see Overdosage (10)], and this risk is increased with higher doses or unapproved methods of administration, such as snorting or injection.
Before prescribing methylphenidate hydrochloride extended-release, assess each patient’s risk for abuse, misuse, and addiction. Educate patients and their families about these risks, proper storage of the drug, and proper disposal of any unused drug. Throughout methylphenidate hydrochloride extended-release treatment, reassess each patient’s risk of abuse, misuse, and addiction and frequently monitor for signs and symptoms of abuse, misuse, and addiction [see Warnings and Precautions (5.1) and Drug Abuse and dependence (9.2)].
WARNING: ABUSE, MISUSE, AND ADDICTION
See full prescribing information for complete boxed warning.
Methylphenidate hydrochloride extended-release has a high potential for abuse and misuse, which can lead to the development of a substance use disorder, including addiction. Misuse and abuse of CNS stimulants, including methylphenidate hydrochloride extended-release , can result in overdose and death(5.1 ,9.2 ,10) :
- Before prescribing methylphenidate hydrochloride extended-release , assess each patient’s risk for abuse, misuse, and addiction.
- Educate patients and their families about these risks, proper storage of the drug, and proper disposal of any unused drug.
- Throughout treatment, reassess each patient’s risk and frequently monitor for signs and symptoms of abuse, misuse, and addiction.
Recent Major Changes
Boxed Warning                                                                       10/2023 Dosage and Administration(2.1 ,2.2)                                      10/2023 Warnings and Precautions(5.1 ,5.2 ,5.8 ,5.9 ,5.10)                10/2023
1 Indications And Usage
Methylphenidate hydrochloride extended-release capsules are indicated for the treatment of Attention Deficit Hyperactivity Disorder (ADHD) in pediatric patients 6 to 15 years of age.
Methylphenidate hydrochloride extended-release capsules are a central nervous system (CNS) stimulant indicated for the treatment of Attention Deficit Hyperactivity Disorder (ADHD) in pediatric patients 6 to 15 years of age.(1)
2 Dosage And Administration
- Take orally once daily in the morning, before breakfast.
- Swallow whole with the aid of liquids, or sprinkle contents onto a small amount of applesauce and give immediately.
- Do not crush or chew the capsule or capsule contents.
(2.1) - Recommended starting dose is 20 mg once daily. Dosage may be increased 10 mg to 20 mg at weekly intervals; do not exceed 60 mg per day.
(2.2) 2.1 Pretreatment Screening
Prior to treating patients with methylphenidate hydrochloride extended-release capsules, assess:
- for the presence of cardiac disease (i.e., perform a careful history, family history of sudden death or ventricular arrhythmia, and physical exam) [see Warnings and Precautions (5.10)].
- the family history and clinically evaluate patients for motor or verbal tics or Tourette’s syndrome before initiating methylphenidate hydrochloride extended-release capsules [see Warnings and Precautions (5.10)].
2.2 DosageRecommendations
The recommended starting dose of methylphenidate hydrochloride extended-release capsules is 20 mg once daily. Dosage may be adjusted in weekly 10 mg to 20 mg increments to the maximum recommended dose of 60 mg per day.
Dosage should be individualized according to the needs and responses of the patient.
2.3 AdministrationInstructions
Administer methylphenidate hydrochloride extended-release capsules orally once daily in the morning, before breakfast.
Swallow the capsule whole with the aid of liquids. Alternatively, open the capsule and sprinkle the contents onto a small amount (tablespoon) of applesauce and administer immediately. Do not store for future use. Drink fluids following the intake of the sprinkled capsule contents with applesauce. The capsules and the capsule contents must not be crushed or chewed.
2.4 Dosage Reductionand Discontinuation
If paradoxical aggravation of symptoms or other adverse reactions occur, reduce dosage or, if necessary, discontinue methylphenidate hydrochloride extended-release capsules. If improvement is not observed after appropriate dosage adjustment over a one-month period, discontinue methylphenidate hydrochloride extended-release capsules.
3 Dosage Forms And Strengths
- Methylphenidate hydrochloride extended-release capsules, 10 mg are green cap and white body, opaque capsules, imprinted with ‚ÄėCP‚Äô over ‚Äė401‚Äô on the cap and ‚Äė10 mg‚Äô on the body.
- Methylphenidate hydrochloride extended-release capsules, 20 mg are blue cap and white body, opaque capsules, imprinted with ‚ÄėCP‚Äô over ‚Äė402‚Äô on the cap and ‚Äė20 mg‚Äô on the body.
- Methylphenidate hydrochloride extended-release capsules, 30 mg are brown cap and white body, opaque capsules, imprinted with ‚ÄėCP‚Äô over ‚Äė403‚Äô on the cap and ‚Äė30 mg‚Äô on the body.
- Methylphenidate hydrochloride extended-release capsules, 40 mg are yellow cap and white body, opaque capsules, imprinted with ‚ÄėCP‚Äô over ‚Äė404‚Äô on the cap and ‚Äė40 mg‚Äô on the body.
- Methylphenidate hydrochloride extended-release capsules, 50 mg are navy blue cap and white body, opaque capsules, imprinted with ‚ÄėCP‚Äô over ‚Äė405‚Äô on the cap and ‚Äė50 mg‚Äô on the body.
- Methylphenidate hydrochloride extended-release capsules, 60 mg are white opaque capsule imprinted with ‚ÄėCP‚Äô over ‚Äė406‚Äô on the cap and ‚Äė60 mg‚Äô on the body.
Extended-release capsules: 10 mg, 20 mg, 30 mg, 40 mg, 50 mg, 60 mg. (3 )
4 Contraindications
Methylphenidate hydrochloride extended-release capsules are contraindicated in patients with:
- known hypersensitivity to methylphenidate or other component of methylphenidate hydrochloride extended-release capsules. Angioedema has been reported in patients treated with methylphenidate hydrochloride extended-release capsules. Anaphylactic reactions have been reported in patients treated with other methylphenidate products [see Adverse Reactions (6)].
- Concomitant treatment with monoamine oxidase inhibitors (MAOIs), or within 14 days following discontinuation of treatment with an MAOI, because of the risk of hypertensive crisis [see Drug Interactions (7)].
- Methylphenidate hydrochloride extended-release capsules contain sucrose. Therefore, patients with hereditary problems of fructose intolerance, glucose-galactose malabsorption, or sucrase-isomaltase insufficiency should not take this medicine.
- Known hypersensitivity to methylphenidate or other components of methylphenidate hydrochloride extended-release capsules. (
4 )- Concurrent treatment with a monoamine oxidase inhibitor (MAOI), or use of an MAOI within the preceding 14 days. (
4 )- Use in patients with patients with hereditary problems of fructose intolerance, glucose-galactose malabsorption, or sucrase-isomaltase insufficiency. (
4 )
 
5 Warnings And Precautions
- Risks to Patients with Serious Cardiac Disease: Avoid use in patients with known structural cardiac abnormalities, cardiomyopathy, serious cardiac arrhythmias, coronary artery disease, or other serious cardiac disease.
(5.2) - Increased Blood Pressure and Heart Rate: Monitor blood pressure and pulse.
(5.3) - Psychiatric Adverse Reactions: Prior to initiating methylphenidate hydrochloride extended-release, screen patients for risk factors for developing a manic episode. If new psychotic or manic symptoms occur, consider discontinuing methylphenidate hydrochloride extended-release.
(5.4) - Priapism: If abnormally sustained or frequent and painful erections occur, patients should seek immediate medical attention.
(5.5) - Peripheral Vasculopathy, including Raynaud’s Phenomenon: Careful observation for digital changes is necessary during methylphenidate hydrochloride extended-release treatment. Further clinical evaluation (e.g., rheumatology referral) may be appropriate for patients who develop signs or symptoms of peripheral vasculopathy.
(5.6) - Long-Term Suppression of Growth in Pediatric Patients: Closely monitor growth (height and weight) in pediatric patients. Pediatric patients not growing or gaining height or weight as expected may need to have their treatment interrupted.
(5.7) - Acute Angle Closure Glaucoma: Methylphenidate hydrochloride extended-release-treated patients considered at risk for acute angle closure glaucoma (e.g., patients with significant hyperopia) should be evaluated by an ophthalmologist.
(5.8) - Increased Intraocular Pressure (IOP) and Glaucoma: Prescribe methylphenidate hydrochloride extended-release to patients with open-angle glaucoma or abnormally increased IOP only if the benefit of treatment is considered to outweigh the risk. Closely monitor patients with a history of increased IOP or open angle glaucoma.
(5.9) - Motor and Verbal Tics, and Worsening of Tourette’s Syndrome: Before initiating methylphenidate hydrochloride extended-release, assess the family history and clinically evaluate patients for tics or Tourette’s syndrome. Regularly monitor patients for the emergence or worsening of tics or Tourette’s syndrome. Discontinue treatment if clinically appropriate.
(5.10) 5.1 Abuse, Misuse, and Addiction
Methylphenidate hydrochloride extended-release has a high potential for abuse and misuse. The use of methylphenidate hydrochloride extended-release exposes individuals to the risks of abuse and misuse, which can lead to the development of a substance use disorder, including addiction. Methylphenidate hydrochloride extended-release can be diverted for non-medical use into illicit channels or distribution [see Drug Abuse and Dependence (9.2)]. Misuse and abuse of CNS stimulants, including methylphenidate hydrochloride extended-release, can result in overdose and death [see Overdosage (10)], and this risk is increased with higher doses or unapproved methods of administration, such as snorting or injection.
Before prescribing methylphenidate hydrochloride extended-release, assess each patient’s risk for abuse, misuse, and addiction. Educate patients and their families about these risks and proper disposal of any unused drug. Advise patients to store methylphenidate hydrochloride extended-release in a safe place, preferably locked, and instruct patients to not give methylphenidate hydrochloride extended-release to anyone else. Throughout methylphenidate hydrochloride extended-release treatment, reassess each patient’s risk of abuse, misuse, and addiction and frequently monitor for signs and symptoms of abuse, misuse, and addiction.
5.2 Risks to Patients with Serious Cardiac Disease
Sudden death has been reported in patients with structural cardiac abnormalities or other serious cardiac disease who were treated with CNS stimulants at the recommended dosage.
Avoid methylphenidate hydrochloride extended-release use in patients with known structural cardiac abnormalities, cardiomyopathy, serious cardiac arrhythmia, coronary artery disease, or other serious cardiac problems.
5.3 Increased Blood Pressure and Heart Rate
CNS stimulants cause an increase in blood pressure (mean increase approximately 2 mmHg to 4 mmHg) and heart rate (mean increase approximately 3 bpm to 6 bpm). Some patients may have larger increases.
Monitor all methylphenidate hydrochloride extended-release-treated patients for hypertension and tachycardia.
5.4 PsychiatricAdverse Reactions
Exacerbation of Pre-Existing Psychosis
CNS stimulants may exacerbate symptoms of behavior disturbance and thought disorder in patients with a pre-existing psychotic disorder.
Induction of a Manic Episode in Patients with Bipolar Disorder
CNS stimulants may induce a manic or mixed episode in patients. Prior to initiating methylphenidate hydrochloride extended-release treatment, screen patients for risk factors for developing a manic episode (e.g., comorbid or history of depressive symptoms or a family history of suicide, bipolar disorder, or depression).
New Psychotic or Manic Symptoms
CNS stimulants, at recommended dosages, may cause psychotic or manic symptoms (e.g., hallucinations, delusional thinking, or mania) in patients without a prior history of psychotic illness or mania. In a pooled analysis of multiple short-term, placebo-controlled studies of CNS stimulants, psychotic or manic symptoms occurred in approximately 0.1% of CNS stimulant-treated patients, compared to 0% of placebo-treated patients. If such symptoms occur, consider discontinuing methylphenidate hydrochloride extended-release.
5.5 Priapism
Prolonged and painful erections, sometimes requiring surgical intervention, have been reported with methylphenidate use in both adult and pediatric male patients. Although priapism was not reported with methylphenidate initiation, it developed after some time on methylphenidate, often subsequent to an increase in dosage. Priapism also occurred during methylphenidate withdrawal (drug holidays or during discontinuation).
Methylphenidate hydrochloride extended-release-treated patients who develop abnormally sustained or frequent and painful erections should seek immediate medical attention.
5.6 PeripheralVasculopathy, including Raynauds Phenomenon
CNS stimulants, including methylphenidate hydrochloride extended-release, used to treat ADHD are associated with peripheral vasculopathy, including Raynaud’s phenomenon. Signs and symptoms are usually intermittent and mild; however, sequelae have included digital ulceration and/or soft tissue breakdown. Effects of peripheral vasculopathy, including Raynaud’s phenomenon, were observed in post-marketing reports and at the therapeutic dosages of CNS stimulants in all age groups throughout the course of treatment. Signs and symptoms generally improved after dosage reduction in or discontinuation of the CNS stimulant.
Careful observation for digital changes is necessary during methylphenidate hydrochloride extended-release treatment. Further clinical evaluation (e.g., rheumatology referral) may be appropriate for methylphenidate hydrochloride extended-release-treated patients who develop signs of symptoms of peripheral vasculopathy.
5.7 Long-Term Suppression of Growth in Pediatric Patients
CNS stimulants have been associated with weight loss and slowing of growth rate in pediatric patients.
Careful follow-up of weight and height in children ages 7 to 10 years who were randomized to either methylphenidate or non-medication treatment groups over 14 months, as well as in naturaulic subgroups of newly methylphenidate-treated and non-medication treated children over 36 months (to the ages of 10 to 13 years), suggests that pediatric patients who received methylphenidate treatment for 7 days per week throughout the year had a temporary slowing in growth rate (on average, a total of about 2 cm less growth in height and 2.7 kg less growth in weight over 3 years), without evidence of growth rebound during this development period.
Closely monitor growth (weight and height) in methylphenidate hydrochloride extended-release-treated pediatric patients. Pediatric patients who are not growing or gaining height or weight as expected may need to have their treatment interrupted.
5.8 Acute Angle Closure Glaucoma
There have been reports of angle closure glaucoma associated with methylphenidate treatment. Although the mechanism is not clear, methylphenidate hydrochloride extended-release-treated patients considered at risk for acute angle closure glaucoma (e.g., patients with significant hyperopia) should be evaluated by an ophthalmologist.
5.9 Increased Intraocular Pressure and Glaucoma
There have been reports of an elevation of intraocular pressure (IOP) associated with methylphenidate treatment [see Adverse Reactions (6.2)].
Prescribe methylphenidate hydrochloride extended-release to patients with open-angle glaucoma or abnormally increased IOP only if the benefit of treatment is considered to outweigh the risk. Closely monitor methylphenidate hydrochloride extended-release-treated patients with a history of abnormally increased IOP or open angle glaucoma.
5.10 Motor and Verbal Tics, and Worsening of Tourettes Syndrome
CNS stimulants, including methylphenidate, have been associated with the onset or exacerbation of motor and verbal tics. Worsening of Tourette’s syndrome has also been reported [see Adverse Reactions (6.2)].
Before initiating methylphenidate hydrochloride extended-release, assess the family history and clinically evaluate patients for tics or Tourette’s syndrome. Regularly monitor methylphenidate hydrochloride extended-release -treated patients for the emergence or worsening of tics or Tourette’s syndrome, and discontinue treatment if clinically appropriate.
6 Adverse Reactions
The following are discussed in more detail in other sections of the labeling:
- Abuse, Misuse, and Addiction [see Warnings and Precautions (5.1), Drug Abuse and Dependence (9.2, 9.3)]
- Hypersensitivity to Methylphenidate and Other Component of Methylphenidate Hydrochloride Extended-Release Capsules [see Contraindications (4)]
- Hypertensive Crisis when Used Concomitantly with MAOIs [see Contraindications (4) and  Drug Interactions (7)]
- Risks to Patients with Serious Cardiac Disease [see Warnings and Precautions (5.2)]
- Increased Blood Pressure and Heart Rate [see Warnings and Precautions (5.3)]
- Psychiatric Adverse Reactions [see Warnings and Precautions (5.4)]
- Priapism [see Warnings and Precautions (5.5)]
- Peripheral Vasculopathy, including Raynaud’s Phenomenon [see Warnings and Precautions (5.6)]
- Long-Term Suppression of Growth in Pediatric Patients [see Warnings and Precautions (5.7)]
- Acute Angle Closure Glaucoma [see Warnings and Precautions (5.8)]
- Increased Intraocular Pressure and Glaucoma [see Warnings and Precautions (5.9)]
- Motor and Verbal Tics, and Worsening of Tourette’s Syndrome [see Warnings and Precautions (5.10)]
The most common adverse reactions (‚Č• 5% and twice the rate of placebo) were anorexia and insomnia. (6.1 )
To report SUSPECTED ADVERSE REACTIONS, contact Amneal Pharmaceuticals at 1-877-835-5472 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
6.1 ClinicalTrials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
Clinical trials experience with methylphenidate hydrochloride extended-release included 188 pediatric patients 6 to 15 years old with ADHD exposed to methylphenidate hydrochloride extended-release. Patients received methylphenidate hydrochloride extended-release 20 mg, 40 mg, and/or 60 mg per day. The 188 patients were evaluated in the following studies: Study 1, a 3-week placebo-controlled clinical study consisting of a total of 314 pediatric patients (ages 6 to 15 years; methylphenidate hydrochloride extended-release n=155); Study 2, a placebo-controlled, crossover clinical study consisting of 25 pediatric patients (ages 7 to 12 years); and Study 3, an uncontrolled clinical study consisting of 8 pediatric patients (ages 6 to 10 years).
Adverse Reactions Leading to Discontinuation of Treatment
In the 3-week placebo-controlled, parallel-group trial, two methylphenidate hydrochloride extended-release-treated patients (1%) and no placebo-treated patients discontinued due to an adverse reaction (rash and pruritus; and headache, abdominal pain, and dizziness, respectively).
Most Common Adverse Reactions
The most common adverse reactions that occurred in 5% or more of patients treated with methylphenidate hydrochloride extended-release in a pool of Studies 1, 2 and 3 (ages 6 to 15 years) where the incidence in patients treated with methylphenidate hydrochloride extended-release was at least twice the incidence in placebo-treated patients were anorexia and insomnia.
Adverse reactions that occurred in ‚Č• 5% of patients treated with methylphenidate hydrochloride extended-release and greater than placebo in pooled Studies 1, 2, and 3 are presented in Table 2:
Table 2: Adverse Reactions (‚Č• 5% and Greater than Placebo) in Pediatric Patients Ages 6 to 15 Years Receiving Methylphenidate Hydrochloride Extended-Release in Pooled Three to Four Week Trials
 Body System Preferred Term 
 Methylphenidate Hydrochloride Extended-Release  
(n=188)
%
Placebo
(n=190)
%
 General  Headache  12  8  Abdominal Pain (stomachache)  7  4  Digestive System  Anorexia  9  2  Nervous System  Insomnia  5  2 6.2 Post-marketingExperience
The following adverse reactions have been identified during post-marketing use of methylphenidate hydrochloride extended-release and other methylphenidate hydrochloride products. Because these reactions are reported voluntarily from a population of uncertain size, it is not possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Adverse Reactions with Methylphenidate Hydrochloride Extended-Release
Blood and the lymphatic system disorders: thrombocytopenia
Cardiac disorders: cardiac arrest, sudden death
Immune system disorders: angioedema
Musculoskeletal and connective tissue disorders: rhabdomyolysis
Psychiatric disorders: abnormal behavior, aggression, anxiety, irritability, obsessive-compulsive disorder, suicidal behavior (including completed suicide), libido changes, serotonin syndrome in combination with serotonergic drugs
Nervous System Disorder: migraine, reversible ischemic neurological deficit, bruxism
Skin and subcutaneous tissue disorders: fixed drug eruption
Vascular disorders: peripheral coldness, Raynaud’s phenomenon
 
Adverse Reactions with Other Methylphenidate Hydrochloride Products
Blood and the lymphatic system disorders: leukopenia, anemia, pancytopenia
Cardiac disorders: palpitations; increased blood pressure, tachycardia, angina pectoris, cardiac arrhythmia, myocardial infarction, bradycardia, extrasystole
Eye disorders: blurred vision, difficulties in visual accommodation, diplopia, increased intraocular pressure, mydriasis
Gastrointestinal disorders: nausea, abdominal pain, dry mouth, vomiting, dyspepsia, diarrhea, constipation
General Disorders: fatigue, hyperpyrexia
Hepatobiliary disorders: abnormal liver function, ranging from transaminase elevation to severe hepatic injury
Immune system disorders: hypersensitivity, including anaphylaxis, auricular swelling, bullous conditions, eruptions, exanthemas
Infections and infestations: nasopharyngitis
Metabolism and nutrition disorders: decreased appetite, reduced weight gain and suppression of growth during prolonged use in pediatric patients
Musculoskeletal and connective tissue disorders: arthralgia, muscle cramps, myalgia, muscle twitching
Nervous System Disorder: nervousness, dizziness, headache, dyskinesia, including choreoatheetoid movements, drowsiness, tremor, convulsions, cerebrovascular disorders (including vasculitis, cerebral hemorrhages and cerebrovascular accidents), serotonin syndrome in combination with serotonergic drugs, motor and verbal tics
Psychiatric disorders: depressed mood, restlessness, agitation, psychosis (sometimes with visual and tactile hallucinations), affect liability, mania, disorientation
Renal and urinary disorders: hematuria
Reproductive system and breast disorders: gynecomastia
Respiratory, thoracic and mediastinal disorders: pharyngolaryngeal pain, dyspnea, cough
Skin and subcutaneous tissue disorders: scalp hair loss, hyperhidrosis, angioneurotic edema, erythema, exfoliative dermatitis, thrombocytopenic purpura, urticaria, erythema multiforme rash
Urogenital disorders: priapism
Vascular disorders: isolated cases of cerebral arteritis and/or occlusion
7 Drug Interactions
Table 3 presents clinically important drug interactions with methylphenidate hydrochloride extended-release.
 
Table 3: Clinically Important Drug Interactions with Methylphenidate Hydrochloride Extended-Release
Monoamine Oxidase Inhibitors (MAOI)
Clinical Impact:
Concomitant use of MAOIs and CNS stimulants, including methylphenidate hydrochloride extended-release, can cause hypertensive crisis. Potential outcomes include death, stroke, myocardial infarction, aortic dissection, ophthalmological complications, eclampsia, pulmonary edema, and renal failure [see Contraindications (4)].
Intervention:
Concomitant use of methylphenidate hydrochloride extended-release with monoamine oxidase inhibitors (MAOIs) or within 14 days after discontinuing MAOI treatment is contraindicated.
Antihypertensive Drugs
Clinical Impact:
Methylphenidate hydrochloride extended-release may decrease the effectiveness of drugs used to treat hypertension [see Warnings and Precautions (5.3)].
Intervention:
Adjust the dosage of the antihypertensive drug as needed.
Halogenated Anesthetics Clinical Impact: Concomitant use of halogenated anesthetics and methylphenidate hydrochloride extended-release may increase the risk of sudden blood pressure and heart rate increase during surgery. Intervention: Monitor blood pressure and avoid use of methylphenidate hydrochloride extended-release in patients being treated with anesthetics on the day of surgery.
Risperidone
Clinical Impact:
Combined use of methylphenidate with risperidone when there is a change, whether an increase or decrease, in dosage of either or both medications, may increase the risk of extrapyramidal symptoms (EPS).
Intervention:
Monitor for signs of EPS.
- Antihypertensive Drugs: Monitor blood pressure. Adjust dosage of antihypertensive drug as needed. (
7 )
8 Use In Specific Populations
8.1 Pregnancy
There is a pregnancy exposure registry that monitors pregnancy outcomes in women exposed to ADHD medications, including methylphenidate hydrochloride extended-release, during pregnancy. Healthcare providers are encouraged to register patients by calling the National Pregnancy Registry for Psychostimulants at 1-866-961-2388.
Risk Summary
Published studies and post-marketing reports on methylphenidate use during pregnancy have not identified a drug-associated risk of major birth defects, miscarriage or adverse maternal or fetal outcomes. There may be risks to the fetus associated with the use of CNS stimulants use during pregnancy (see Clinical Considerations).
No effects on morphological development were observed in embryo-fetal development studies with oral administration of methylphenidate to pregnant rats and rabbits during organogenesis at doses up to 10 and 15 times, respectively, the maximum recommended human dose (MRHD) of 60 mg/day given to adolescents on a mg/m2 basis. However, spina bifida was observed in rabbits at a dose 53 times the MRHD given to adolescents. A decrease in pup body weight was observed in a pre-and post-natal development study with oral administration of methylphenidate to rats throughout pregnancy and lactation at doses 6 times the MRHD given to adolescents (see Data).
The estimated background risk of major birth defects and miscarriage for the indicated population is unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
Clinical Considerations
Fetal/Neonatal Adverse Reactions
CNS stimulants, such as methylphenidate hydrochloride extended-release, can cause vasoconstriction and thereby decrease placental perfusion. No fetal and/or neonatal adverse reactions have been reported with the use of therapeutic doses of methylphenidate during pregnancy; however, premature delivery and low birth weight infants have been reported in amphetamine-dependent mothers.
Animal Data
In embryo-fetal development studies conducted in rats and rabbits, methylphenidate was administered orally at doses of up to 75 and 200 mg/kg/day, respectively, during the period of organogenesis. Malformations (increased incidence of fetal spina bifida) were observed in rabbits at the highest dose, which is approximately 52 times the MRHD of 60 mg/day given to adolescents on a mg/m2 basis. The no effect level for embryo-fetal development in rabbits was 60 mg/kg/day (15 times the MRHD given to adolescents on a mg/m2 basis). There was no evidence of morphological development effects in rats, although increased incidences of fetal skeletal variations were seen at the highest dose level (10 times the MRHD of 60 mg/day given to adults on a mg/m2 basis), which was also maternally toxic. The no effect level for embryo-fetal development in rats was 25 mg/kg/day (3 times the MRHD on a mg/m2 basis). When methylphenidate was administered to rats throughout pregnancy and lactation at doses of up to 45 mg/kg/day, offspring body weight gain was decreased at the highest dose (6 times the MRHD of 60 mg/day given to adults on a mg/m2 basis), but no other effects on postnatal development were observed. The no effect level for pre-and postnatal development in rats was 15 mg/kg/day (~2 times the MRHD given to adolescents on a mg/m2 basis).
8.2 Lactation
Risk Summary
Limited published literature, based on milk sampling from seven mothers reports that methylphenidate is present in human milk, which resulted in infant doses of 0.16% to 0.7% of the maternal weight-adjusted dosage and a milk/plasma ratio ranging between 1.1 and 2.7. There are no reports of adverse effects on the breastfed infant and no effects on milk production. Long-term neurodevelopmental effects on infants from stimulant exposure are unknown. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for methylphenidate hydrochloride extended-release and any potential adverse effects on the breastfed infant from methylphenidate hydrochloride extended-release or from the underlying maternal condition.
Clinical Considerations
Monitor breastfeeding infants for adverse reactions, such as agitation, insomnia, anorexia, and reduced weight gain.
8.4 Pediatric Use
The safety and effectiveness of methylphenidate hydrochloride extended-release for the treatment of ADHD have been established in pediatric patients 6 to 15 years of age. The safety and effectiveness of methylphenidate hydrochloride extended-release in pediatric patients younger than 6 years of age have not been established. Long-term efficacy of methylphenidate in pediatric patients have not been established.
Long-Term Suppression of Growth
Growth should be monitored during treatment with stimulants, including methylphenidate hydrochloride extended-release. Pediatric patients who are not growing or gaining weight as expected may need to have their treatment interrupted [see Warnings and Precautions (5.6)].
Juvenile Animal Toxicity Data
In a study conducted in young rats, methylphenidate was administered orally at doses of up to 100 mg/kg/day for 9 weeks, starting early in the postnatal period (postnatal Day 7) and continuing through sexual maturity (postnatal Week 10). When these animals were tested as adults (postnatal Weeks 13 to 14), decreased spontaneous locomotor activity was observed in males and females previously treated with 50 mg/kg/day (approximately 6 times the MRHD on a mg/m2 basis) or greater, and a deficit in the acquisition of a specific learning task was seen in females exposed to the highest dose (12 times the MRHD on a mg/m2 basis). The no effect level for juvenile neurobehavioral development in rats was 5 mg/kg/day (half the MRHD on a mg/m2 basis). The clinical significance of the long-term behavioral effects observed in rats is unknown.
8.5 Geriatric Use
Methylphenidate hydrochloride extended-release has not been studied in patients over the age of 65 years.
9 Drug Abuse And Dependence
9.1 ControlledSubstance
Methylphenidate hydrochloride extended-release capsules contain methylphenidate hydrochloride, a Schedule II controlled substance.
9.2 Abuse
Methylphenidate hydrochloride extended-release has a high potential for abuse and misuse which can lead to the development of a substance use disorder, including addiction [see Warnings and Precautions (5.1)]. Methylphenidate hydrochloride extended-release can be diverted for non-medical use into illicit channels or distribution.
Abuse is the intentional non-therapeutic use of a drug, even once, to achieve a desired psychological or physiological effect. Misuse is the intentional use, for therapeutic purposes, of a drug by an individual in a way other than prescribed by a health care provider or for whom it was not prescribed. Drug addiction is a cluster of behavioral, cognitive, and physiological phenomena that may include a strong desire to take the drug, difficulties in controlling drug use (e.g., continuing drug use despite harmful consequences, giving a higher priority to drug use than other activities and obligations), and possible tolerance or physical dependence.
Misuse and abuse of methylphenidate may cause increased heart rate, respiratory rate, or blood pressure; sweating; dilated pupils; hyperactivity; restlessness; insomnia; decreased appetite; loss of coordination; tremors; flushed skin; vomiting; and/or abdominal pain. Anxiety, psychosis, hostility, aggression, and suicidal or homicidal ideation have also been observed with CNS stimulants abuse and/or misuse. Misuse and abuse of CNS stimulants, including methylphenidate hydrochloride extended-release, can result in overdose and death [see Overdosage (10)], and this risk is increased with higher doses or unapproved methods of administration, such as snorting or injection.
9.3Dependence
Physical Dependence
Methylphenidate hydrochloride extended-release may produce physical dependence. Physical dependence is a state that develops as a result of physiological adaptation in response to repeated drug use, manifested by withdrawal signs and symptoms after abrupt discontinuation or a significant dose reduction of a drug.
Withdrawal signs symptoms after abrupt discontinuation or dose reduction following prolonged use of CNS stimulants including methylphenidate hydrochloride extended-release include dysphoric mood; depression; fatigue; vivid; unpleasant dreams; insomnia or hypersomnia; increased appetite; and psychomotor retardation or agitation.
Tolerance
Methylphenidate hydrochloride extended-release may produce tolerance. Tolerance is a physiological state characterized by a reduced response to a drug after repeated administration (i.e., a higher dose of a drug is required to produce the same effect that was once obtained at a lower dose).
10 Overdosage
Clinical Effects of Overdose
Overdose of CNS stimulants is characterized by the following sympathomimetic effects:
- Cardiovascular effects including tachyarrhythmias, and hypertension or hypotension. Vasospasm, myocardial infarction, or aortic dissection may precipitate sudden cardiac death. Takotsubo cardiomyopathy may develop.
- CNS effects including psychomotor agitation, confusion, and hallucinations. Serotonin syndrome, seizures, cerebral vascular accidents, and coma may occur.
- Life-threatening hyperthermia (temperatures greater than 104¬ļF) and rhabdomyolysis may develop.
Overdose Management
Consider the possibility of multiple drug ingestion. The pharmacokinetic profile of methylphenidate hydrochloride extended-release should be considered when treating patients with overdose. Because methylphenidate has a large volume of distribution and is rapidly metabolized, dialysis is not useful. Consider contacting the Poison Help line (1-800-222-1222) or a medical toxicologist for additional overdose management recommendations.
11 Description
Methylphenidate hydrochloride extended-release capsules contains methylphenidate hydrochloride, USP, a CNS stimulant. The extended-release capsules comprise both immediate-release (IR) and extended-release (ER) beads such that 30% of the dose is provided by the IR component and 70% of the dose is provided by the ER component. Methylphenidate hydrochloride extended-release capsules are available in six strengths containing 10 mg (3 mg IR; 7 mg ER), 20 mg (6 mg IR; 14 mg ER), 30 mg (9 mg IR; 21 mg ER), 40 mg (12 mg IR; 28 mg ER), 50 mg (15 mg IR; 35 mg ER), or 60 mg (18 mg IR; 42 mg ER) of methylphenidate hydrochloride, USP for oral administration.
Chemically, methylphenidate hydrochloride, USP is d,l (racemic)-threo-methyl őĪ-phenyl-2-piperidineacetate hydrochloride. Its empirical formula is C14H19NO2‚ÄĘHCl. Its structural formula is:
Methylphenidate hydrochloride, USP is a white, odorless, crystalline powder. Its solutions are acid to litmus. It is freely soluble in water and in methanol, soluble in alcohol, and slightly soluble in chloroform and in acetone. Its molecular weight is 269.77 g/mol.
Methylphenidate hydrochloride extended-release capsules also contain the following inactive ingredients: Sugar spheres, povidone, hydroxypropylmethylcellulose and polyethylene glycol, ethyl cellulose, cetyl alcohol, sodium lauryl sulfate, dibutyl sebacate, gelatin and titanium dioxide.
The individual capsules contain the following color agents:
10 mg capsules: FD&C Blue No. 2, FDA/E172 Yellow Iron Oxide
20 mg capsules: D&C  Red No. 28, FD&C Blue No. 1, FD&C Green No. 3
30 mg capsules:  FDA/E172 Black Iron Oxide, FDA/E172 Red Iron Oxide, FDA/E172 Yellow Iron Oxide
40 mg capsules:  D&C Yellow No. 10, FD&C Red No. 40
50 mg capsules: D&C Red No. 28, FD&C Green No. 3, FDA/E172 Black Iron Oxide
12 Clinical Pharmacology
12.1 Mechanism of Action
Methylphenidate hydrochloride is a central nervous system (CNS) stimulant. The mode of therapeutic action in ADHD is not known.
12.2 Pharmacodynamics
Methylphenidate is a racemic mixture comprised of the d- and l-threo enantiomers. The d-threo enantiomer is more pharmacologically active than the l-threo enantiomer. Methylphenidate blocks the reuptake of norepinephrine and dopamine into the presynaptic neuron and increases the release of these monoamines into the extraneuronal space.
12.3 Pharmacokinetics
Following one week of once-daily doses of 20 mg or 40 mg methylphenidate hydrochloride extended-release to children aged 7 to 12 years old with ADHD, Cmax and AUC of methylphenidate were approximately proportional to the administered doses.
Absorption
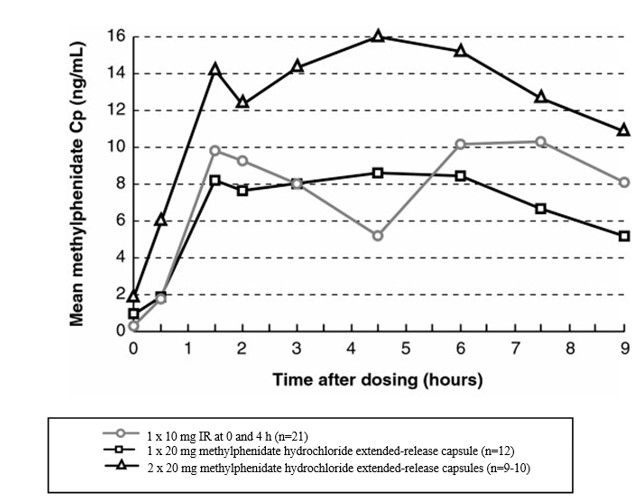
Following administration of methylphenidate hydrochloride extended-release in children aged 7 to 12 years old with ADHD, the plasma concentration time profile of methylphenidate showed two phases of drug release with a sharp, initial slope similar to a methylphenidate immediate-release tablet (median T max1  about 1.5 hours post dose), and a second rising portion approximately three hours later (median T max2  about 4.5 hours post dose)*, followed by a gradual decline (Figure 1). The means for Cmax and area under the curve (AUC) following a dose of 20 mg were slightly lower than those seen with 10 mg of the immediate-release formulation, dosed at 0 and 4 hours.
*25% to 30% of the subjects had only one observed peak (Cmax) concentration of methylphenidate.
Figure 1: Comparison of Immediate Release (IR) and Methylphenidate Hydrochloride Extended-Release Formulations After Repeated Doses of Methylphenidate Hydrochloride in Pediatric Patients 7 to 12 Years of Age with ADHD
Effect of Food
Ingestion of a high-fat meal with methylphenidate hydrochloride extended-release increased the mean Cmax and AUC of methylphenidate by about 30% and 17%, respectively. The presence of food delayed the early peak by approximately 1 hour (range -2 to 5 hours delay) [see Dosage and Administration (2.1)].
The bioavailability (Cmax and AUC) of methylphenidate was unaffected by sprinkling the methylphenidate hydrochloride extended-release capsule contents on applesauce as compared to the intact capsule.
Effect of Alcohol
At an alcohol concentration of 40%, there was an increase in the release rate of methylphenidate in the first hour, resulting in 84% of the methylphenidate being released. The results with the 60 mg capsule are considered to be representative of the other available capsule strengths [see Drug Interactions (7)].
Distribution
Plasma protein binding is 10% to 33%. The volume of distribution was 2.65 ¬Ī 1.11 L/kg for d- methylphenidate and 1.80 ¬Ī 0.91 L/kg for l- methylphenidate.
Elimination
The mean terminal half-life (t1/2) of methylphenidate following administration of methylphenidate hydrochloride extended-release capsules (t1/2=6.8 hours) is longer than the mean terminal t1/2 following administration of methylphenidate hydrochloride immediate-release tablets (t1/2=2.9 hours) and methylphenidate hydrochloride extended-release tablets (t1/2=3.4 hours) in healthy adult volunteers.
Metabolism
In vitro studies showed that methylphenidate was not metabolized by cytochrome P450 isoenzymes. Methylphenidate is metabolized primarily by deesterification to alpha-phenyl-piperidine acetic acid (ritalinic acid), which has little or no pharmacologic activity.
Excretion
After oral administration of radiolabeled methylphenidate in humans, about 90% of the radioactivity was recovered in urine. The main urinary metabolite was ritalinic acid, accounting for approximately 80% of the dose.
Specific Populations
Male and Female Patients
The pharmacokinetics of methylphenidate after a single-dose of methylphenidate hydrochloride extended-release were similar between adult men and women.
Racial or Ethnic Groups
The influence of race on the pharmacokinetics of methylphenidate after methylphenidate hydrochloride extended-release administration has not been studied.
Pediatric Patients
The pharmacokinetics of methylphenidate after methylphenidate hydrochloride extended-release administration has not been studied in children less than 6 years of age.
Patients with Renal Impairment
Methylphenidate hydrochloride extended-release has not been studied in patients with renal insufficiency. Since renal clearance is not an important route of methylphenidate clearance, and the major metabolite (ritalinic acid), has little or no pharmacologic activity, renal insufficiency is expected to have minimal effect on the pharmacokinetics of methylphenidate hydrochloride extended-release.
Patients with Hepatic Impairment
Methylphenidate hydrochloride extended-release has not been studied in patients with hepatic insufficiency. Hepatic impairment is expected to have minimal effect on the pharmacokinetics of methylphenidate since it is metabolized primarily to ritalinic acid by nonmicrosomal hydrolytic esterases that are widely distributed throughout the body.
Drug Interaction Studies
In vitro studies showed that methylphenidate did not inhibit cytochrome P450 isoenzymes at clinically observed plasma drug concentrations.
13 Nonclinical Toxicology
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis
In a lifetime carcinogenicity study carried out in B6C3F1 mice, methylphenidate caused an increase in hepatocellular adenomas and, in males only, an increase in hepatoblastomas, at a daily dose of approximately 60 mg/kg per day. This dose is approximately 2 times the maximum recommended human dose (MRHD) of 60 mg/day given to children on a mg/m2 basis. Hepatoblastoma is a relatively rare rodent malignant tumor type. There was no increase in total malignant hepatic tumors. The mouse strain used is sensitive to the development of hepatic tumors, and the significance of these results to humans is unknown.
Methylphenidate did not cause any increases in tumors in a lifetime carcinogenicity study carried out in F344 rats; the highest dose used was approximately 45 mg/kg/day, which is approximately 4 times the MRHD (children) on a mg/m2 basis.
In a 24-week carcinogenicity study in the transgenic mouse strain p53+/-, which is sensitive to genotoxic carcinogens, there was no evidence of carcinogenicity. Male and female mice were fed diets containing the same concentration of methylphenidate as in the lifetime carcinogenicity study; the high-dose groups were exposed to 60 mg/kg to 74 mg/kg per day of methylphenidate.
Mutagenesis
Methylphenidate was not mutagenic in the in vitro Ames reverse mutation assay, in the in vitro mouse lymphoma cell forward mutation assay, or in the in vitro chromosomal aberration assay using human lymphocytes. Sister chromatid exchanges and chromosome aberrations were increased, indicative of a weak clastogenic response, in an in vitro assay in cultured Chinese Hamster Ovary cells. Methylphenidate was negative in vivo in males and females in the mouse bone marrow micronucleus assay.
Impairment of Fertility
Methylphenidate did not impair fertility in male or female mice that were fed diets containing the drug in an 18-week continuous breeding study. The study was conducted at doses up to 160 mg/kg per day, approximately 10 times the maximum recommended human dose of 60 mg/day given to adolescents on a mg/m2 basis.
14 Clinical Studies
Methylphenidate hydrochloride extended-release was evaluated in a double-blind, parallel-group, placebo-controlled trial in which 321 untreated or previously treated pediatric patients with a DSM-IV diagnosis of Attention Deficit Hyperactivity Disorder (ADHD), 6 to 15 years of age, received a single morning dose for up to 3 weeks. Patients were required to have the combined or predominantly hyperactive-impulsive subtype of ADHD; patients with the predominantly inattentive subtype were excluded. Patients randomized to the methylphenidate hydrochloride extended-release group received 20 mg daily for the first week. Their dosage could be increased weekly to a maximum of 60 mg by the third week, depending on individual response to treatment.
The patient’s regular school teacher completed the teachers’ version of the Conners’ Global Index Scale (TCGIS), a scale for assessing ADHD symptoms, in the morning and again in the afternoon on three alternate days of each treatment week. The primary efficacy endpoint was determined by the average of the total scores for the 10-li TCGIS completed by the classroom teacher in the morning and again in the afternoon on the three observation days during the last week of double-blind therapy. Patients treated with methylphenidate hydrochloride extended-release showed a statistically significant improvement in symptom scores from baseline over patients who received placebo (see Figure 2). Separate analyses of TCGIS scores in the morning and afternoon revealed superiority in improvement with methylphenidate hydrochloride extended-release over placebo during both time periods (see Figure 3).
Figure 2: Least Squares Mean Change from Baseline in TCGIS Total Score in Pediatric Patients 6 to 15 years of Age with ADHD
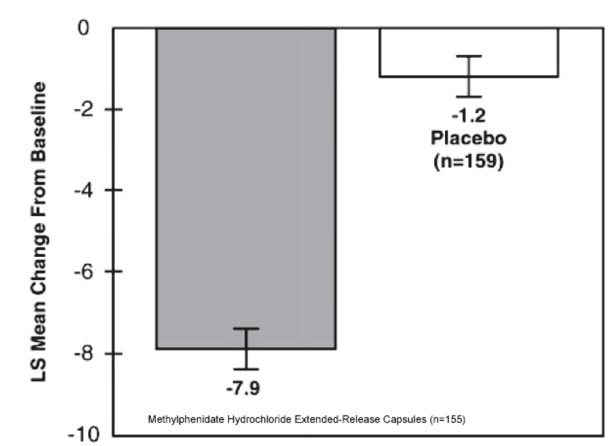
 
Figure 3: Least Squares Mean Change from Baseline in TCGIS Total Score in Pediatric Patients 6 to 15 years of Age with ADHD: Morning (AM) and Afternoon (PM)
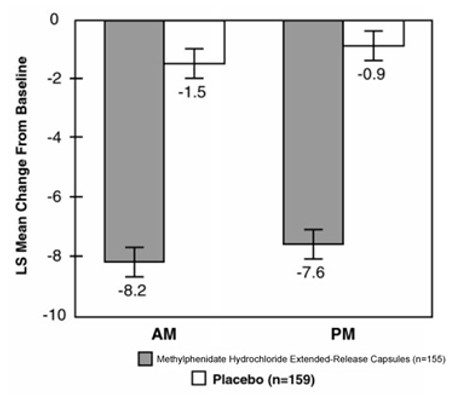
* FIGURES 2 & 3: Last observation carried forward analysis at week 3.
Error bars represent the standard error of the mean.
16 How Supplied/storage And Handling
How Supplied
Methylphenidate hydrochloride extended-release capsules are available in six strengths:
Methylphenidate hydrochloride extended-release capsules, 10 mg are green cap and white body, opaque capsules, imprinted with ‚ÄėCP‚Äô over ‚Äė401‚Äô on the cap and ‚Äė10 mg‚Äô on the body.
They are available as:
Bottles of 100:                        NDC 0115-1736-01
Methylphenidate hydrochloride extended-release capsules, 20 mg are blue cap and white body, opaque capsules, imprinted with ‚ÄėCP‚Äô over ‚Äė402‚Äô on the cap and ‚Äė20 mg‚Äô on the body.
They are available as:
Bottles of 100:                        NDC 0115-1737-01
Methylphenidate hydrochloride extended-release capsules, 30 mg are brown cap and white body, opaque capsules, imprinted with ‚ÄėCP‚Äô over ‚Äė403‚Äô on the cap and ‚Äė30 mg‚Äô on the body.
They are available as:
Bottles of 100:                        NDC 0115-1738-01
Methylphenidate hydrochloride extended-release capsules, 40 mg are yellow cap and white body, opaque capsules, imprinted with ‚ÄėCP‚Äô over ‚Äė404‚Äô on the cap and ‚Äė40 mg‚Äô on the body.
They are available as:
Bottles of 100:                        NDC 0115-1739-01
Methylphenidate hydrochloride extended-release capsules, 50 mg are navy blue cap and white body, opaque capsules, imprinted with ‚ÄėCP‚Äô over ‚Äė405‚Äô on the cap and ‚Äė50 mg‚Äô on the body.
They are available as:
Bottles of 100:                        NDC 0115-1740-01
Methylphenidate hydrochloride extended-release capsules, 60 mg are white opaque capsule imprinted with ‚ÄėCP‚Äô over ‚Äė406‚Äô on the cap and ‚Äė60 mg‚Äô on the body.
They are available as:
Bottles of 100:                        NDC 0115-1741-01
Storage and Handling
Store at 20¬į to 25¬įC (68¬į to 77¬įF); excursions permitted between 15¬į to 30¬įC (59¬į to 86¬įF) [see USP Controlled Room Temperature].
Keep out of the reach of children.
17 Patient Counseling Information
Advise the patient to read the FDA-approved patient labeling (Medication Guide).
Abuse, Misuse, and Addiction
Educate patients and their families about the risks of abuse, misuse, and addiction of methylphenidate hydrochloride extended-release, which can lead to overdose and death, and proper disposal of any unused drug [see Warnings and Precautions (5.1), Drug Abuse and Dependence (9.2), Overdosage (10)]. Advise patients to store methylphenidate hydrochloride extended-release in a safe place, preferably locked, and instruct patients to not give methylphenidate hydrochloride extended-release to anyone else.
Administration Instructions
Instruct patients and their caregivers that the methylphenidate hydrochloride extended-release capsules and the capsule contents must not be crushed or chewed. Instruct patients that the capsule may be swallowed whole, or alternatively, the capsule may be opened and the capsule contents sprinkled onto a small amount (tablespoon) of applesauce and given immediately, and not stored for future use [see Dosage and Administration (2.3)].
Risks to Patients with Serious Cardiac Disease
Advise patients that there are potential risks to patients with serious cardiac disease, including sudden death, with methylphenidate hydrochloride extended-release use. Instruct patients to contact a healthcare provider immediately if they develop symptoms such as exertional chest pain, unexplained syncope, or other symptoms suggestive of cardiac disease [see Warnings and Precautions (5.2)].
Increased Blood Pressure and Heart Rate
Instruct patients and their caregivers that methylphenidate hydrochloride extended-release can cause elevations of their blood pressure and pulse rate [see Warnings and Precautions (5.3)].
Psychiatric Adverse Reactions
Advise patients and their caregivers that methylphenidate hydrochloride extended-release, at recommended doses, can cause psychotic or manic symptoms, even in patients without a prior history of psychotic symptoms or mania [see Warnings and Precautions (5.4)].
Priapism
Advise patients and their caregivers of the possibility of painful or prolonged penile erections (priapism). Instruct the patient to seek immediate medical attention in the event of priapism [see Warnings and Precautions (5.5)].
Circulation Problems in Fingers and Toes (peripheral vasculopathy, including Raynaud’s phenomenon)
- Instruct patients about the risk of peripheral vasculopathy, including Raynaud’s phenomenon, and associated signs and symptoms: fingers or toes may feel numb, cool, painful, and/or may change color from pale, to blue, to red.
- Instruct patients to report to their physician any new numbness, pain, skin color change, or sensitivity to temperature in fingers or toes.
- Instruct patients to call their physician immediately with any signs of unexplained wounds appearing on fingers or toes. Further clinical evaluation (e.g., rheumatology referral) may be appropriate for certain patients [see Warnings and Precautions (5.6)].
Long-Term Suppression of Growth in Pediatric Patients
Advise patients and their caregivers that methylphenidate hydrochloride extended-release can cause slowing of growth and weight loss [see Warnings and Precautions (5.7)].
Increased Intraocular Pressure (IOP) and Glaucoma
Advise patients what IOP and glaucoma may occur during treatment with methylphenidate hydrochloride extended-release [see Warnings and Precautions (5.9)].
Motor and Verbal Tics, and Worsening of Tourette's Syndrome
Advise patients that motor and verbal tics and worsening of Tourette’s Syndrome may occur during treatment with methylphenidate hydrochloride extended-release. Instruct patients to notify their healthcare provider if emergence of new tics or worsening of tics or Tourette’s syndrome occurs [see Warnings and Precautions (5.10)].
Pregnancy Registry
Inform patients that there is a pregnancy exposure registry that monitors pregnancy outcomes in women exposed to methylphenidate hydrochloride extended-release during pregnancy [see Use in Specific Populations (8.1)].
Alcohol Use
Advise patients to avoid alcohol while taking methylphenidate hydrochloride extended-release. Consumption of alcohol while taking methylphenidate hydrochloride extended-release may result in a more rapid release of the dose of methylphenidate [see Drug Interactions (7)].
Manufactured by: Amneal Pharmaceuticals of New York, LLC Brookhaven, NY 11719
Distributed by: Amneal Pharmaceuticals LLC Bridgewater, NJ 08807
Rev. 11-2023-03
Dispense with Medication Guide available at: documents.amneal.com/mg/methylphenidate-hcl-er-cap.pdf
Medication Guide
Methylphenidate Hydrochloride (meth" il fen' i date hye" droe klor' ide)
Extended-Release Capsules, CII
 What is the most important information I should know about  methylphenidate hydrochloride extended-release capsules ?
Methylphenidate hydrochloride extended-release capsules may cause serious side effects, including:
- Abuse, misuse, and addiction. Methylphenidate hydrochloride extended-release capsules, has a high chance for abuse and misuse and may lead to substance use problems, including addiction. Misuse and abuse of methylphenidate hydrochloride extended-release capsules, other methylphenidate containing medicines, and amphetamine containing medicines, can lead to overdose and death. The risk of overdose and death is increased with higher doses of methylphenidate hydrochloride extended-release capsules or when it is used in ways that are not approved, such as snorting or injection.
- Your healthcare provider should check your child’s risk for abuse, misuse, and addiction before starting treatment with methylphenidate hydrochloride extended-release capsules and will monitor your child during treatment.
- Methylphenidate hydrochloride extended-release capsules may lead to physical dependence after prolonged use, even if taken as directed by your healthcare provider.
- Do not give methylphenidate hydrochloride extended-release capsules to anyone else. See ‚ÄúWhat is methylphenidate hydrochloride extended-release capsules?‚ÄĚ for more information.
Keep methylphenidate hydrochloride extended-release capsules in a safe place and properly dispose of any unused medicine. See ‚ÄúHow should I store methylphenidate hydrochloride extended-release capsules?‚ÄĚ for more information.
Tell your healthcare provider if your child has ever abused or been dependent on alcohol, prescription medicines, or street drugs.
- Risks for people with serious heart disease. Sudden death has happened in people who have heart defects or other serious heart disease.
Your healthcare provider should check your child carefully for heart problems before starting treatment with methylphenidate hydrochloride extended-release capsules. Tell your healthcare provider if your child has any heart problems, heart disease, or heart defects.
Call your healthcare provider or go to the nearest hospital emergency room right away if your child has any signs of heart problems such as chest pain, shortness of breath, or fainting during treatment with  methylphenidate hydrochloride extended-release capsules.
- Increased blood pressure and heart rate.
Your healthcare provider should check your child’s blood pressure and heart rate regularly during treatment with methylphenidate hydrochloride extended-release capsules.
- Mental (psychiatric) problems, including:
- new or worse behavior and thought problems
- new or worse bipolar illness
- new psychotic symptoms (such as hearing voices, or seeing or believing things that are not real) or new manic symptoms
Tell your healthcare provider about any mental problems your child has, or about a family history of, suicide, bipolar illness, or depression.
Call your healthcare provider right away if your child has any new or worsening mental symptoms or problems during treatment with  methylphenidate hydrochloride extended-release capsules, especially hearing voices, seeing or believing things that are not real, or new manic symptoms.
What are  methylphenidate hydrochloride extended-release capsules?
Methylphenidate hydrochloride extended-release capsules are a prescription medicine used for the treatment of Attention Deficit Hyperactivity Disorder (ADHD) in children 6 to 15 years of age. Methylphenidate hydrochloride extended-release capsules may help increase attention and decrease impulsiveness and hyperactivity in people with ADHD.
It is not known if methylphenidate hydrochloride extended-release capsules are safe and effective for use in children younger than 6 years of age or older than 15 years of age.
Methylphenidate hydrochloride extended-release capsules are a federally controlled substance (CII) because it contains methylphenidate that can be a target for people who abuse prescription medicines or street drugs. Keep methylphenidate hydrochloride extended-release capsules in a safe place to protect it from theft. Never give your methylphenidate hydrochloride extended-release capsules to anyone else, because it may cause death or harm them. Selling or giving away methylphenidate hydrochloride extended-release capsules may harm others and is against the law.
Who should not take  methylphenidate hydrochloride extended-release capsules?
Your child should not take methylphenidate hydrochloride extended-release capsules if your child:
- is allergic to methylphenidate hydrochloride or any of the ingredients in methylphenidate hydrochloride extended-release capsules. See the end of this Medication Guide for a complete ul of ingredients in methylphenidate hydrochloride extended-release capsules.
- has a rare inherited problem with the breaking down, absorbing, and processing of certain types of sugar in the body. Methylphenidate hydrochloride extended-release capsules contain a type of sugar called sucrose.
- is taking, or has stopped taking within the past 14 days, a medicine called a monoamine oxidase inhibitor (MAOI).
Before starting methylphenidate hydrochloride extended-release capsules tell your healthcare provider about all your child’s medical conditions, including if your child:
- has heart problems, heart disease, heart defects, or high blood pressure
- has mental problems including psychosis, mania, bipolar illness, or depression or has a family history of suicide, bipolar illness, or depression
- has circulation problems in fingers and toes
- have eye problems, including increased pressure in your eye, glaucoma, or problems with your close-up vision (farsightedness)
- have or had repeated movements or sounds (tics) or Tourette’s syndrome, or have a family history of tics or Tourette’s syndrome
- is pregnant or plan to become pregnant. It is not known if methylphenidate hydrochloride extended-release capsules will harm the unborn baby.
- There is a pregnancy registry for females who are exposed to methylphenidate hydrochloride extended-release capsules during pregnancy. The purpose of the registry is to collect information about the health of females exposed to methylphenidate hydrochloride extended-release capsules and their baby. If you or your child becomes pregnant during treatment with methylphenidate hydrochloride extended-release capsules, talk to your healthcare provider about registering with the National Pregnancy Registry for Psychostimulants at 1-866-961-2388.
- is breastfeeding or plan to breastfeed. Methylphenidate hydrochloride passes into breast milk. Talk to your healthcare provider about the best way to feed the baby during treatment with methylphenidate hydrochloride extended-release capsules.
Tell your healthcare provider about all the medicines that your child takes, including prescription and over-the-counter medicines, vitamins, and herbal supplements.
Methylphenidate hydrochloride extended-release capsules and some medicines may interact with each other and cause serious side effects. Sometimes the doses of other medicines will need to be changed during treatment with methylphenidate hydrochloride extended-release capsules. Your healthcare provider will decide whether methylphenidate hydrochloride extended-release capsules can be taken with other medicines.
Especially tell your healthcare provider if your child takes a medicine used to treat depression called a monoamine oxidase inhibitor (MAOI).
Know the medicines that your child takes. Keep a ul of the medicines with you to show your healthcare provider and pharmacist. Your child should not start taking any new medicines during treatment with methylphenidate hydrochloride extended-release capsules without talking to your healthcare provider first.
 How should methylphenidate hydrochloride extended-release capsules be taken?
- Take methylphenidate hydrochloride extended-release capsules exactly as prescribed by your healthcare provider.
- Your healthcare provider may change the dose if needed.
- Take methylphenidate hydrochloride extended-release capsules 1 time each day in the morning before breakfast.
- Swallow methylphenidate hydrochloride extended-release capsules whole with water or other liquids.
- If methylphenidate hydrochloride extended-release capsules cannot be swallowed whole, the capsule may be opened and the contents sprinkled onto a tablespoonful of applesauce.
- Follow with a drink of water or other liquid.
- Do not chew the applesauce and medicine mixture.
- Swallow all the applesauce and medicine mixture right away. Do not store the applesauce and medicine mixture.
If your child takes too much  methylphenidate hydrochloride extended-release capsules, call your healthcare provider or Poison Help line at 1-800-222-1222 or go to the nearest hospital emergency room right away.
What should be avoided during treatment with  methylphenidate hydrochloride extended-release capsules?
Avoid drinking alcohol during treatment with methylphenidate hydrochloride extended-release capsules. This may cause a faster release of the methylphenidate hydrochloride extended-release capsules medicine.
 What are the possible side effects of  methylphenidate hydrochloride extended-release capsules?
Methylphenidate hydrochloride extended-release capsules may cause serious side effects, including:
- See ‚ÄúWhat is the most important information I should know about¬† methylphenidate hydrochloride extended-release capsules?‚ÄĚ
- Painful and prolonged erections (priapism). Priapism has happened in males who take products that contain methylphenidate. If your child develops priapism, get medical help right away.
- Circulation problems in fingers and toes (peripheral vasculopathy, including Raynaud’s phenomenon). Signs and symptoms may include:
- fingers or toes may feel numb, cool, painful
- fingers or toes may change color from pale, to blue, to red
Tell your healthcare provider if your child has numbness, pain, skin color change, or sensitivity to temperature in the fingers or toes.
Call your healthcare provider right away if your child has any signs of unexplained wounds appearing on the fingers or toes during treatment with methylphenidate hydrochloride extended-release capsules.
- Slowing of growth (height and weight) in children. Children should have their height and weight checked often during treatment with methylphenidate hydrochloride extended-release capsules. Methylphenidate hydrochloride extended-release capsules treatment may be stopped if your child is not growing or gaining weight.
- Eye problems (increased pressure in the eye and glaucoma). Call your healthcare provider right away if you or your child develop changes in your vision or eye pain, swelling, or redness.
- New or worsening tics or worsening Tourette’s syndrome. Tell your healthcare provider if you or your child get any new or worsening tics or worsening Tourette’s syndrome during treatment with methylphenidate hydrochloride extended-release capsules.
The most common side effects of methylphenidate hydrochloride extended-release capsules include anorexia and trouble sleeping. These are not all the possible side effects of methylphenidate hydrochloride extended-release capsules. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088.
 How should I store  methylphenidate hydrochloride extended-release capsules?
- Store methylphenidate hydrochloride extended-release capsules at 20¬į to 25¬įC (68¬į to 77¬įF); excursions permitted between 15¬į to 30¬įC (59¬į to 86¬įF).
- Store methylphenidate hydrochloride extended-release capsules in a safe place, like a locked cabinet. Protect from light and moisture.
- Dispose of remaining, unused, or expired methylphenidate hydrochloride extended-release capsules by a medicine take-back program at a U.S. Drug Enforcement Administration (DEA) authorized collection site. If no take-back program or DEA authorized collector is available, mix methylphenidate hydrochloride extended-release capsules with an undesirable, nontoxic substance such as dirt, cat litter, or used coffee grounds to make it less appealing to children and pets. Place the mixture in a container such as a sealed plastic bag and throw away methylphenidate hydrochloride extended-release capsules in the household trash. Visit www.fda.gov/drugdisposal for additional information on disposal of unused medicines.
Keep methylphenidate hydrochloride extended-release capsules and all medicines out of the reach of children.
 General information about the safe and effective use of  methylphenidate hydrochloride extended-release capsules.
Medicines are sometimes prescribed for purposes other than those uled in a Medication Guide. Do not use methylphenidate hydrochloride extended-release capsules for a condition for which it was not prescribed. Do not give methylphenidate hydrochloride extended-release capsules to other people, even if they have the same symptoms. It may harm them and it is against the law. You can ask your healthcare provider or pharmacist for information about methylphenidate hydrochloride extended-release capsules that is written for healthcare professionals.
 What are the ingredients in  methylphenidate hydrochloride extended-release capsules?
Active Ingredient: Methylphenidate hydrochloride, USP
Inactive Ingredients: sugar spheres, povidone, hydroxypropylmethylcellulose and polyethylene glycol, ethyl cellulose, cetyl alcohol, sodium lauryl sulfate, dibutyl sebacate, gelatin, and titanium dioxide.
The individual capsules contain the following coloring agents:
10 mg capsules: FD&C Blue No. 2, FDA/E172 Yellow Iron Oxide
20 mg capsules: D&C Red No. 28, FD&C Blue No. 1, FD&C Green No. 3
30 mg capsules: FDA/E172 Black Iron Oxide, FDA/E172 Red Iron Oxide, FDA/E172 Yellow Iron Oxide
40 mg capsules: D&C Yellow No. 10, FD&C Red No. 40
50 mg capsules: D&C Red No. 28, FD&C Green No. 3, FDA/E172 Black Iron Oxide
For more information about methylphenidate hydrochloride extended-release capsules call 1-877-835-5472 .
This Medication Guide has been approved by the U.S. Food and Drug Administration.
Manufactured by: Amneal Pharmaceuticals of New York, LLC Brookhaven, NY 11719
Distributed by: Amneal Pharmaceuticals LLC Bridgewater, NJ 08807
Rev. 11-2023-03 Dispense with Medication Guide available at: documents.amneal.com/mg/methylphenidate-hcl-er-cap.pdf
Principal Display Panel
NDC 0115-1736-01
Methylphenidate Hydrochloride Extended-Release Capsules, 10 mg (CII)
Rx only100 Capsules

NDC 0115-1737-01
Methylphenidate Hydrochloride Extended-Release Capsules, 20 mg (CII)
Rx only100 Capsules

NDC 0115-1738-01
Methylphenidate Hydrochloride Extended-Release Capsules, 30 mg (CII)
Rx only100 Capsules
NDC 0115-1739-01
Methylphenidate Hydrochloride Extended-Release Capsules, 40 mg (CII)
Rx only100 Capsules
NDC 0115-1740-01
Methylphenidate Hydrochloride Extended-Release Capsules, 50 mg (CII)
Rx only100 Capsules
NDC 0115-1741-01
Methylphenidate Hydrochloride Extended-Release Capsules, 60 mg (CII)
Rx only100 Capsules
DISCLAIMER:
"This tool does not provide medical advice, and is for informational and educational purposes only, and is not a substitute for professional medical advice, treatment or diagnosis. Call your doctor to receive medical advice. If you think you may have a medical emergency, please dial 911."
"Do not rely on openFDA to make decisions regarding medical care. While we make every effort to ensure that data is accurate, you should assume all results are unvalidated. We may limit or otherwise restrict your access to the API in line with our Terms of Service."
"This product uses publicly available data from the U.S. National Library of Medicine (NLM), National Institutes of Health, Department of Health and Human Services; NLM is not responsible for the product and does not endorse or recommend this or any other product."
PillSync may earn a commission via links on our site
