CADUET® (amlodipine besylate and atorvastatin calcium) tablets
combine the calcium channel blocker amlodipine besylate with the lipid-lowering
agent atorvastatin calcium.
The amlodipine besylate component of CADUET is chemically described as
3-ethyl-5-methyl
(±)-2-[(2-aminoethoxy)methyl]-4-(o-chlorophenyl)-1,4-dihydro-6-methyl-3,5-pyridinedicarboxylate,
monobenzenesulphonate. Its empirical formula is C20H25ClN2O5•C6H6O3S.
The atorvastatin calcium component of CADUET is chemically described as
[R-(R*, R*)]-2-(4-fluorophenyl)-β,
δ-dihydroxy-5-(1-methylethyl)-3-phenyl-4-[(phenylamino)carbonyl]-1H-pyrrole-1-heptanoic
acid, calcium salt (2:1) trihydrate. Its empirical formula is (C33H34FN2O5)2Ca•3H2O. The structural formulae for amlodipine besylate and atorvastatin calcium are
shown below. CADUET contains amlodipine besylate, a white to off-white crystalline powder,
and atorvastatin calcium, also a white to off-white crystalline powder.
Amlodipine besylate has a molecular weight of 567.1 and atorvastatin calcium has
a molecular weight of 1209.42. Amlodipine besylate is slightly soluble in water
and sparingly soluble in ethanol. Atorvastatin calcium is insoluble in aqueous
solutions of pH 4 and below. Atorvastatin calcium is very slightly soluble in
distilled water, pH 7.4 phosphate buffer, and acetonitrile; slightly soluble in
ethanol, and freely soluble in methanol.
CADUET tablets are formulated for oral administration in the following
strength combinations:
Table 1. CADUET Tablet Strengths
2.5 mg/10mg
2.5 mg/20mg
2.5 mg/40mg
5 mg/10mg
5 mg/20mg
5 mg/40mg
5 mg/80mg
10 mg/10 mg
10 mg/20 mg
10 mg/40 mg
10 mg/80 mg
amlodipineequivalent(mg)
2.5
2.5
2.5
5
5
5
5
10
10
10
10
atorvastatinequivalent(mg)
10
20
40
10
20
40
80
10
20
40
80
Each tablet also contains calcium carbonate, croscarmellose sodium,
microcrystalline cellulose, pregelatinized starch, polysorbate 80, hydroxypropyl
cellulose, purified water, colloidal silicon dioxide (anhydrous), magnesium
stearate, Opadry® II White 85F28751 (polyvinyl alcohol, titanium dioxide, PEG
3000 and talc) or Opadry® II Blue 85F10919 (polyvinyl alcohol, titanium dioxide,
PEG 3000, talc and FD&C blue #2). Combinations of atorvastatin with 2.5 mg
and 5 mg amlodipine are film coated white, and combinations of atorvastatin with
10 mg amlodipine are film coated blue.
Clinical Pharmacology
Mechanism of ActionCADUET CADUET is a combination of two drugs, a dihydropyridine calcium
channel blocker amlodipine and an HMG-CoA reductase inhibitor atorvastatin. The
amlodipine component of CADUET inhibits the transmembrane influx of calcium ions
into vascular smooth muscle and cardiac muscle. The atorvastatin component of
CADUET is a selective, competitive inhibitor of HMG-CoA reductase (statin), the
rate-limiting enzyme that converts 3-hydroxy-3-methylglutaryl-coenzyme A to
mevalonate, a precursor of sterols, including cholesterol. Amlodipine Experimental data suggest that amlodipine binds to both
dihydropyridine and nondihydropyridine binding sites. The contractile processes
of cardiac muscle and vascular smooth muscle are dependent upon the movement of
extracellular calcium ions into these cells through specific ion channels.
Amlodipine inhibits calcium ion influx across cell membranes selectively, with a
greater effect on vascular smooth muscle cells than on cardiac muscle cells.
Negative inotropic effects can be detected in vitro
but such effects have not been seen in intact animals at therapeutic doses.
Serum calcium concentration is not affected by amlodipine.
Amlodipine is a peripheral arterial vasodilator that acts directly on
vascular smooth muscle to cause a reduction in peripheral vascular resistance
and reduction in blood pressure.
The precise mechanisms by which amlodipine relieves angina have not been
fully delineated, but are thought to include the following:
Exertional Angina: In patients with exertional angina, amlodipine reduces the
total peripheral resistance (afterload) against which the heart works and
reduces the rate pressure product, and thus myocardial oxygen demand, at any
given level of exercise.
Vasospastic Angina: Amlodipine has been demonstrated to block constriction
and restore blood flow in coronary arteries and arterioles in response to
calcium, potassium epinephrine, serotonin, and thromboxane A2 analog in experimental animal models and in human coronary
vessels in vitro. This inhibition of coronary spasm
is responsible for the effectiveness of amlodipine in vasospastic (Prinzmetal's
or variant) angina. Atorvastatin Cholesterol and triglycerides circulate in the bloodstream as
part of lipoprotein complexes. With ultracentrifugation, these complexes
separate into HDL (high-density lipoprotein), IDL (intermediate-density
lipoprotein), LDL (low-density lipoprotein), and VLDL (very-low-density
lipoprotein) fractions. Triglycerides (TG) and cholesterol in the liver are
incorporated into VLDL and released into the plasma for delivery to peripheral
tissues. LDL is formed from VLDL and is catabolized primarily through the
high-affinity LDL receptor.
Clinical and pathologic studies show that elevated plasma levels of total
cholesterol (total-C), LDL-cholesterol (LDL-C), and apolipoprotein B (apo B)
promote human atherosclerosis and are risk factors for developing cardiovascular
disease, while increased levels of HDL-C are associated with a decreased
cardiovascular risk.
Epidemiologic investigations have established that cardiovascular morbidity
and mortality vary directly with the level of total-C and LDL-C, and inversely
with the level of HDL-C.
In animal models, atorvastatin lowers plasma cholesterol and lipoprotein
levels by inhibiting HMG-CoA reductase and cholesterol synthesis in the liver
and by increasing the number of hepatic LDL receptors on the cell-surface to
enhance uptake and catabolism of LDL; atorvastatin also reduces LDL production
and the number of LDL particles.
Atorvastatin reduces total-C, LDL-C, and apo B in patients with homozygous
and heterozygous familial hypercholesterolemia (FH), nonfamilial forms of
hypercholesterolemia, and mixed dyslipidemia. Atorvastatin also reduces VLDL-C
and TG and produces variable increases in HDL-C and apolipoprotein A-1.
Atorvastatin reduces total-C, LDL-C, VLDL-C, apo B, TG, and non-HDL-C, and
increases HDL-C in patients with isolated hypertriglyceridemia. Atorvastatin
reduces intermediate density lipoprotein cholesterol (IDL-C) in patients with
dysbetalipoproteinemia.
Like LDL, cholesterol-enriched triglyceride-rich lipoproteins, including
VLDL, intermediate density lipoprotein (IDL), and remnants, can also promote
atherosclerosis. Elevated plasma triglycerides are frequently found in a triad
with low HDL-C levels and small LDL particles, as well as in association with
non-lipid metabolic risk factors for coronary heart disease. As such, total
plasma TG has not consistently been shown to be an independent risk factor for
CHD. Furthermore, the independent effect of raising HDL or lowering TG on the
risk of coronary and cardiovascular morbidity and mortality has not been
determined. Pharmacokinetics and MetabolismAbsorptionStudies with amlodipine After oral administration of therapeutic doses of amlodipine
alone, absorption produces peak plasma concentrations between 6 and 12 hours.
Absolute bioavailability has been estimated to be between 64% and 90%. Studies with atorvastatin After oral administration alone, atorvastatin is rapidly
absorbed; maximum plasma concentrations occur within 1 to 2 hours. Extent of
absorption increases in proportion to atorvastatin dose. The absolute
bioavailability of atorvastatin (parent drug) is approximately 14% and the
systemic availability of HMG-CoA reductase inhibitory activity is approximately
30%. The low systemic availability is attributed to presystemic clearance in
gastrointestinal mucosa and/or hepatic first-pass metabolism. Plasma
atorvastatin concentrations are lower (approximately 30% for Cmax and AUC)
following evening drug administration compared with morning. However, LDL-C
reduction is the same regardless of the time of day of drug administration (see
DOSAGE AND
ADMINISTRATION). Studies with CADUET Following oral administration of CADUET peak plasma
concentrations of amlodipine and atorvastatin are seen at 6 to 12 hours and 1 to
2 hours post dosing, respectively. The rate and extent of absorption
(bioavailability) of amlodipine and atorvastatin from CADUET are not
significantly different from the bioavailability of amlodipine and atorvastatin
administered separately (see above).
The bioavailability of amlodipine from CADUET was not affected by food. Food
decreases the rate and extent of absorption of atorvastatin from CADUET by
approximately 32% and 11%, respectively, as it does with atorvastatin when given
alone. LDL-C reduction is similar whether atorvastatin is given with or without
food. DistributionStudies with amlodipine Ex vivo studies have shown that
approximately 93% of the circulating amlodipine drug is bound to plasma proteins
in hypertensive patients. Steady-state plasma levels of amlodipine are reached
after 7 to 8 days of consecutive daily dosing. Studies with atorvastatin Mean volume of distribution of atorvastatin is approximately 381
liters. Atorvastatin is ≥98% bound to plasma proteins. A blood/plasma ratio of
approximately 0.25 indicates poor drug penetration into red blood cells. Based
on observations in rats, atorvastatin calcium is likely to be secreted in human
milk (see CONTRAINDICATIONS, Pregnancy and
Lactation, and PRECAUTIONS, Nursing Mothers). MetabolismStudies with amlodipine Amlodipine is extensively (about 90%) converted to inactive
metabolites via hepatic metabolism. Studies with atorvastatin Atorvastatin is extensively metabolized to ortho- and
parahydroxylated derivatives and various beta-oxidation products. In vitro inhibition of HMG-CoA reductase by ortho- and
parahydroxylated metabolites is equivalent to that of atorvastatin.
Approximately 70% of circulating inhibitory activity for HMG-CoA reductase is
attributed to active metabolites. In vitro studies
suggest the importance of atorvastatin metabolism by cytochrome P450 3A4,
consistent with increased plasma concentrations of atorvastatin in humans
following coadministration with erythromycin, a known inhibitor of this isozyme
(see PRECAUTIONS, Drug
Interactions). In animals, the ortho-hydroxy metabolite undergoes
further glucuronidation. ExcretionStudies with amlodipine Elimination from the plasma is biphasic with a terminal
elimination half-life of about 30–50 hours. Ten percent of the parent amlodipine
compound and 60% of the metabolites of amlodipine are excreted in the
urine. Studies with atorvastatin Atorvastatin and its metabolites are eliminated primarily in bile
following hepatic and/or extra-hepatic metabolism; however, the drug does not
appear to undergo enterohepatic recirculation. Mean plasma elimination half-life
of atorvastatin in humans is approximately 14 hours, but the half-life of
inhibitory activity for HMG-CoA reductase is 20 to 30 hours due to the
contribution of active metabolites. Less than 2% of a dose of atorvastatin is
recovered in urine following oral administration. Specific PopulationsGeriatricStudies with amlodipine Elderly patients have decreased clearance of amlodipine with a
resulting increase in AUC of approximately 40–60%, and a lower initial dose of
amlodipine may be required. Studies with atorvastatin Plasma concentrations of atorvastatin are higher (approximately
40% for Cmax and 30% for AUC) in healthy elderly subjects (age ≥65 years) than
in young adults. Clinical data suggest a greater degree of LDL-lowering at any
dose of atorvastatin in the elderly population compared to younger adults (see
PRECAUTIONS, Geriatric Use). PediatricStudies with amlodipine Sixty-two hypertensive patients aged 6 to 17 years received doses
of amlodipine between 1.25 mg and 20 mg. Weight-adjusted clearance and volume of
distribution were similar to values in adults. Studies with atorvastatin Pharmacokinetic data in the pediatric population are not
available. GenderStudies with atorvastatin Plasma concentrations of atorvastatin in women differ from those
in men (approximately 20% higher for Cmax and 10% lower for AUC); however, there
is no clinically significant difference in LDL-C reduction with atorvastatin
between men and women. Renal Impairment Studies with amlodipine The pharmacokinetics of amlodipine are not significantly
influenced by renal impairment. Patients with renal failure may therefore
receive the usual initial amlodipine dose. Studies with atorvastatin Renal disease has no influence on the plasma concentrations or
LDL-C reduction of atorvastatin; thus, dose adjustment of atorvastatin in
patients with renal dysfunction is not necessary (see DOSAGE AND ADMINISTRATION and WARNINGS, Skeletal
Muscle). Hemodialysis While studies have not been conducted in patients with end-stage
renal disease, hemodialysis is not expected to clear atorvastatin or amlodipine
since both drugs are extensively bound to plasma proteins. Hepatic Impairment Atorvastatin is contraindicated in patients with active liver
disease. Studies with amlodipine Elderly patients and patients with hepatic insufficiency have
decreased clearance of amlodipine with a resulting increase in AUC of
approximately 40–60%. Studies with atorvastatin In patients with chronic alcoholic liver disease, plasma
concentrations of atorvastatin are markedly increased. Cmax and AUC are each
4-fold greater in patients with Childs-Pugh A disease. Cmax and AUC of
atorvastatin are approximately 16-fold and 11-fold increased, respectively, in
patients with Childs-Pugh B disease (see CONTRAINDICATIONS). Heart FailureStudies with amlodipine In patients with moderate to severe heart failure, the increase
in AUC for amlodipine was similar to that seen in the elderly and in patients
with hepatic insufficiency. Pharmacokinetic Studies of Atorvastatin and
Co-Administered Drugs
TABLE 2. Effect of Co-administered Drugs on the Pharmacokinetics of Atorvastatin
*Â Â Â Â Data given as x-fold change represent a simple ratio between co-administration
and atorvastatin alone (i.e., 1-fold = no change). Data given as % change
represent % difference relative to atorvastatin alone (i.e., 0% = no change).
†    See WARNINGS, Skeletal Muscle and PRECAUTIONS, Drug Interactions for
clinical significance.
‡    Greater increases in AUC (up to 2.5-fold) and/or Cmax (up to 71%) have been reported
with excessive grapefruit consumption (≥ 750 mL – 1.2 liters per day).
§    Single sample taken 8-16 h post dose.
¶    Due to the dual interaction mechanism of rifampin, simultaneous co-administration of
atorvastatin with rifampin is recommended, as delayed administration of
atorvastatin after administration of rifampin has been associated with a
significant reduction in atorvastatin plasma concentrations.
TABLE 3. Effect of Atorvastatin on the Pharmacokinetics of Co-administered Drugs
Atorvastatin
Co-administered
drug and dosing regimen
Drug/Dose (mg)
Change in AUC
Change in Cmax
80 mg QD for 15 days                  Â
40 mg QD for 22 days                                         Â
Oral contraceptive QD, 2 months     Â
- norethindrone 1 mg
↑ 28%
↑ 23%
- ethinyl estradiol 35µg
↑ 19%
↑ 30%
*Â Â Â Â See PRECAUTIONS, Drug Interactions
for clinical significance.
PharmacodynamicsHemodynamic Effects of Amlodipine Following administration of therapeutic doses to patients with
hypertension, amlodipine produces vasodilation resulting in a reduction of
supine and standing blood pressures. These decreases in blood pressure are not
accompanied by a significant change in heart rate or plasma catecholamine levels
with chronic dosing. Although the acute intravenous administration of amlodipine
decreases arterial blood pressure and increases heart rate in hemodynamic
studies of patients with chronic stable angina, chronic administration of oral
amlodipine in clinical trials did not lead to clinically significant changes in
heart rate or blood pressures in normotensive patients with angina.
With chronic once daily oral administration of amlodipine, antihypertensive
effectiveness is maintained for at least 24 hours. Plasma concentrations
correlate with effect in both young and elderly patients. The magnitude of
reduction in blood pressure with amlodipine is also correlated with the height
of pretreatment elevation; thus, individuals with moderate hypertension
(diastolic pressure 105–114 mmHg) had about a 50% greater response than patients
with mild hypertension (diastolic pressure 90–104 mmHg). Normotensive subjects
experienced no clinically significant change in blood pressures (+1/–2
mmHg).
In hypertensive patients with normal renal function, therapeutic doses of
amlodipine resulted in a decrease in renal vascular resistance and an increase
in glomerular filtration rate and effective renal plasma flow without change in
filtration fraction or proteinuria.
As with other calcium channel blockers, hemodynamic measurements of cardiac
function at rest and during exercise (or pacing) in patients with normal
ventricular function treated with amlodipine have generally demonstrated a small
increase in cardiac index without significant influence on dP/dt or on left
ventricular end diastolic pressure or volume. In hemodynamic studies, amlodipine
has not been associated with a negative inotropic effect when administered in
the therapeutic dose range to intact animals and man, even when co-administered
with beta-blockers to man. Similar findings, however, have been observed in
normals or well-compensated patients with heart failure with agents possessing
significant negative inotropic effects. Electrophysiologic Effects of Amlodipine Amlodipine does not change sinoatrial nodal function or
atrioventricular conduction in intact animals or man. In patients with chronic
stable angina, intravenous administration of 10 mg did not significantly alter
A-H and H-V conduction and sinus node recovery time after pacing. Similar
results were obtained in patients receiving amlodipine and concomitant beta
blockers. In clinical studies in which amlodipine was administered in
combination with beta-blockers to patients with either hypertension or angina,
no adverse effects on electrocardiographic parameters were observed. In clinical
trials with angina patients alone, amlodipine therapy did not alter
electrocardiographic intervals or produce higher degrees of AV blocks. LDL-C Reduction with Atorvastatin Atorvastatin as well as some of its metabolites are
pharmacologically active in humans. The liver is the primary site of action and
the principal site of cholesterol synthesis and LDL clearance. Drug dosage,
rather than systemic drug concentration, correlates better with LDL-C reduction.
Individualization of drug dosage should be based on therapeutic response (see
DOSAGE AND
ADMINISTRATION). Clinical StudiesClinical Studies with AmlodipineAmlodipine Effects in HypertensionAdult Patients The antihypertensive efficacy of amlodipine has been demonstrated
in a total of 15 double-blind, placebo-controlled, randomized studies involving
800 patients on amlodipine and 538 on placebo. Once daily administration
produced statistically significant placebo-corrected reductions in supine and
standing blood pressures at 24 hours postdose, averaging about 12/6 mmHg in the
standing position and 13/7 mmHg in the supine position in patients with mild to
moderate hypertension. Maintenance of the blood pressure effect over the 24-hour
dosing interval was observed, with little difference in peak and trough effect.
Tolerance was not demonstrated in patients studied for up to 1 year. The 3
parallel, fixed doses, dose response studies showed that the reduction in supine
and standing blood pressures was dose-related within the recommended dosing
range. Effects on diastolic pressure were similar in young and older patients.
The effect on systolic pressure was greater in older patients, perhaps because
of greater baseline systolic pressure. Effects were similar in black patients
and in white patients. Pediatric Patients Two-hundred sixty-eight hypertensive patients aged 6 to 17 years
were randomized first to amlodipine 2.5 or 5 mg once daily for 4 weeks and then
randomized again to the same dose or to placebo for another 4 weeks. Patients
receiving 5 mg amlodipine at the end of 8 weeks had lower blood pressure than
those secondarily randomized to placebo. The magnitude of the treatment effect
is difficult to interpret, but it is probably less than 5 mmHg systolic on the 5
mg dose. Adverse events were similar to those seen in adults. Amlodipine Effects in Chronic Stable Angina The effectiveness of 5–10 mg/day of amlodipine in
exercise-induced angina has been evaluated in 8 placebo-controlled, double-blind
clinical trials of up to 6 weeks duration involving 1038 patients (684
amlodipine, 354 placebo) with chronic stable angina. In 5 of the 8 studies,
significant increases in exercise time (bicycle or treadmill) were seen with the
10 mg dose. Increases in symptom-limited exercise time averaged 12.8% (63 sec)
for amlodipine 10 mg, and averaged 7.9% (38 sec) for amlodipine 5 mg. Amlodipine
10 mg also increased time to 1 mm ST segment deviation in several studies and
decreased angina attack rate. The sustained efficacy of amlodipine in angina
patients has been demonstrated over long-term dosing. In patients with angina,
there were no clinically significant reductions in blood pressures (4/1 mmHg) or
changes in heart rate (+0.3 bpm). Amlodipine Effects in Vasospastic Angina In a double-blind, placebo-controlled clinical trial of 4 weeks
duration in 50 patients, amlodipine therapy decreased attacks by approximately
4/week compared with a placebo decrease of approximately 1/week (p less than 0.01). Two
of 23 amlodipine and 7 of 27 placebo patients discontinued from the study due to
lack of clinical improvement. Amlodipine Effects in Documented Coronary Artery
Disease In PREVENT, 825 patients with angiographically documented
coronary artery disease were randomized to amlodipine (5–10 mg once daily) or
placebo and followed for 3 years. Although the study did not show significance
on the primary objective of change in coronary luminal diameter as assessed by
quantitative coronary angiography, the data suggested a favorable outcome with
respect to fewer hospitalizations for angina and revascularization procedures in
patients with CAD.
CAMELOT enrolled 1318 patients with CAD recently documented by angiography,
without left main coronary disease and without heart failure or an ejection
fraction less than 40%. Patients (76% males, 89% Caucasian, 93% enrolled at US sites,
89% with a history of angina, 52% without PCI, 4% with PCI and no stent, and 44%
with a stent) were randomized to double-blind treatment with either amlodipine
(5 – 10 mg once daily) or placebo in addition to standard care that included
aspirin (89%), statins (83%), beta-blockers (74%), nitroglycerin (50%),
anti-coagulants (40%), and diuretics (32%), but excluded other calcium channel
blockers. The mean duration of follow-up was 19 months. The primary endpoint was
the time to first occurrence of one of the following events: hospitalization for
angina pectoris, coronary revascularization, myocardial infarction,
cardiovascular death, resuscitated cardiac arrest, hospitalization for heart
failure, stroke/TIA, or peripheral vascular disease. A total of 110 (16.6%) and
151 (23.1%) first events occurred in the amlodipine and placebo groups
respectively for a hazard ratio of 0.691 (95% CI: 0.540–0.884, p= 0.003). The
primary endpoint is summarized in Figure 1 below. The outcome of this study was
largely derived from the prevention of hospitalizations for angina and the
prevention of revascularization procedures (see Table 4).
Effects in various subgroups are shown in Figure 2.
In a angiographic substudy (n=274) conducted within CAMELOT, there was no
significant difference between amlodipine and placebo on the change of atheroma
volume in the coronary artery as assessed by intravascular ultrasound.
Figure 1: Kaplan-Meier analysis of composite clinical outcomes
for amlodipineversus placeboFigure 2 – Effects on primary endpoint of amlodipine versus
placebo across sub-groups
Table 4 below summarizes the significant composite endpoint and clinical
outcomes from the composites of the primary endpoint. The other components of
the primary endpoint including cardiovascular death, resuscitated cardiac
arrest, myocardial infarction, hospitalization for heart failure, stroke/TIA, or
peripheral vascular disease did not demonstrate a significant difference between
amlodipine and placebo.
Table 4. Incidence of Significant Clinical Outcomes for CAMELOT
*Â Â Â Â Total patients with these events
Amlodipine Effects in Patients with Congestive Heart
Failure Amlodipine has been compared to placebo in four 8–12 week studies
of patients with NYHA class II/III heart failure, involving a total of 697
patients. In these studies, there was no evidence of worsened heart failure
based on measures of exercise tolerance, NYHA classification, symptoms, or LVEF.
In a long-term (follow-up at least 6 months, mean 13.8 months)
placebo-controlled mortality/morbidity study of amlodipine 5–10 mg in 1153
patients with NYHA classes III (n=931) or IV (n=222) heart failure on stable
doses of diuretics, digoxin, and ACE inhibitors, amlodipine had no effect on the
primary endpoint of the study which was the combined endpoint of all-cause
mortality and cardiac morbidity (as defined by life-threatening arrhythmia,
acute myocardial infarction, or hospitalization for worsened heart failure), or
on NYHA classification, or symptoms of heart failure. Total combined all-cause
mortality and cardiac morbidity events were 222/571 (39%) for patients on
amlodipine and 246/583 (42%) for patients on placebo; the cardiac morbid events
represented about 25% of the endpoints in the study.
Another study (PRAISE-2) randomized patients with NYHA class III (80%) or IV
(20%) heart failure without clinical symptoms or objective evidence of
underlying ischemic disease, on stable doses of ACE inhibitor (99%), digitalis
(99%) and diuretics (99%), to placebo (n=827) or amlodipine (n=827) and followed
them for a mean of 33 months. There was no statistically significant difference
between amlodipine and placebo in the primary endpoint of all cause mortality
(95% confidence limits from 8% reduction to 29% increase on amlodipine). With
amlodipine there were more reports of pulmonary edema.
Clinical Studies with Atorvastatin Prevention of Cardiovascular Disease In the Anglo-Scandinavian Cardiac Outcomes Trial (ASCOT), the
effect of atorvastatin on fatal and non-fatal coronary heart disease was
assessed in 10,305 hypertensive patients 40–80 years of age (mean of 63 years),
without a previous myocardial infarction and with TC levels less than or equal to 251 mg/dl (6.5
mmol/l). Additionally all patients had at least 3 of the following
cardiovascular risk factors: male gender (81.1%), age greater than 55 years (84.5%),
smoking (33.2%), diabetes (24.3%), history of CHD in a first-degree relative
(26%), TC:HDL greater than 6 (14.3%), peripheral vascular disease (5.1%), left
ventricular hypertrophy (14.4%), prior cerebrovascular event (9.8%), specific
ECG abnormality (14.3%), proteinuria/albuminuria (62.4%)]. In this double-blind,
placebo-controlled study, patients were treated with anti-hypertensive therapy
(Goal BP less than 140/90 mm Hg for non-diabetic patients; less than 130/80 mm Hg for
diabetic patients) and allocated to either atorvastatin 10 mg daily (n=5168) or
placebo (n=5137), using a covariate adaptive method which took into account the
distribution of nine baseline characteristics of patients already enrolled and
minimized the imbalance of those characteristics across the groups. Patients
were followed for a median duration of 3.3 years.
The effect of 10 mg/day of atorvastatin on lipid levels was similar to that
seen in previous clinical trials.
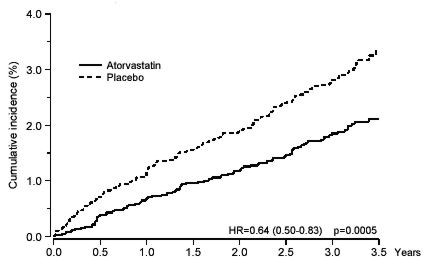
Atorvastatin significantly reduced the rate of coronary events [either fatal
coronary heart disease (46 events in the placebo group vs. 40 events in the
atorvastatin group) or nonfatal MI (108 events in the placebo group vs. 60
events in the atorvastatin group)] with a relative risk reduction of 36% [(based
on incidences of 1.9% for atorvastatin vs. 3.0% for placebo), p=0.0005 (see Figure 3)]. The risk reduction was consistent regardless of
age, smoking status, obesity, or presence of renal dysfunction. The effect of
atorvastatin was seen regardless of baseline LDL levels. Due to the small number
of events, results for women were inconclusive.
Figure 3: Effect of Atorvastatin 10 mg/day on Cumulative
Incidence of NonfatalMyocardial Infarction or Coronary Heart Disease Death
(in ASCOT-LLA) Atorvastatin also significantly decreased the relative risk for
revascularization procedures by 42%. Although the reduction of fatal and
non-fatal strokes did not reach a pre-defined significance level (p 0.01), a
favorable trend was observed with a 26% relative risk reduction (incidences of
1.7% for atorvastatin and 2.3% for placebo). There was no significant difference
between the treatment groups for death due to cardiovascular causes (p=0.51) or
noncardiovascular causes (p=0.17).
In the Collaborative Atorvastatin Diabetes Study (CARDS), the effect of
atorvastatin on cardiovascular disease (CVD) endpoints was assessed in 2838
subjects (94% White, 68% male), ages 40–75 with type 2 diabetes based on WHO
criteria, without prior history of cardiovascular disease and with LDL less than or equal to 160
mg/dL and TG less than or equal to 600 mg/dL. In addition to diabetes, subjects had 1 or more of the
following risk factors: current smoking (23%), hypertension (80%), retinopathy
(30%), or microalbuminuria (9%) or macroalbuminuria (3%). No subjects on
hemodialysis were enrolled in the study. In this multicenter,
placebo-controlled, double-blind clinical trial, subjects were randomly
allocated to either atorvastatin 10 mg daily (1429) or placebo (1411) in a 1:1
ratio and were followed for a median duration of 3.9 years. The primary endpoint
was the occurrence of any of the major cardiovascular events: myocardial
infarction, acute CHD death, unstable angina, coronary revascularization, or
stroke. The primary analysis was the time to first occurrence of the primary
endpoint.
Baseline characteristics of subjects were: mean age of 62 years, mean
HbA1c 7.7%; median LDL-C 120 mg/dL; median TC 207 mg/dL;
median TG 151 mg/dL; median HDL-C 52 mg/dL.
The effect of atorvastatin 10 mg/day on lipid levels was similar to that seen
in previous clinical trials.
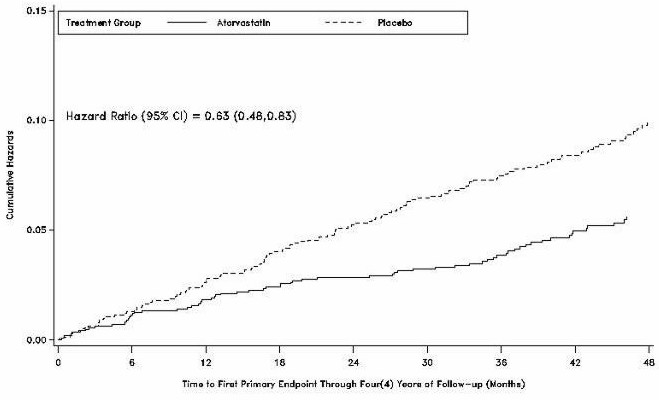
Atorvastatin significantly reduced the rate of major cardiovascular events
(primary endpoint events) (83 events in the atorvastatin group vs 127 events in
the placebo group) with a relative risk reduction of 37%, HR 0.63, 95% CI
(0.48,0.83) (p=0.001) (see Figure 4). An effect of
atorvastatin was seen regardless of age, sex, or baseline lipid levels.
Figure 4. Effect of Atorvastatin 10 mg/day on Time to
Occurrence of MajorCardiovascular Events (myocardial infarction, acute CHD
death, unstable angina,coronary revascularization, or stroke) in
CARDS.
Atorvastatin significantly reduced the risk of stroke by 48% (21 events in
the atorvastatin group vs. 39 events in the placebo group), HR 0.52, 95% CI
(0.31, 0.89) (p=0.016) and reduced the risk of MI by 42% (38 events in the
atorvastatin group vs. 64 events in the placebo group), HR 0.58, 95.1% CI (0.39,
0.86) (p=0.007). There was no significant difference between the treatment
groups for angina, revascularization procedures, and acute CHD death.
There were 61 deaths in the atorvastatin group vs. 82 deaths in the placebo
group, (HR 0.73, p=0.059).
In the Treating to New Targets Study (TNT), the effect of LIPITOR 80 mg/day
vs. LIPITOR 10 mg/day on the reduction in cardiovascular events was assessed in
10,001 subjects (94% white, 81% male, 38% greater than or equal to 65 years) with clinically evident
coronary heart disease who had achieved a target LDL-C level less than 130 mg/dL after
completing an 8-week, open-label, run-in period with LIPITOR 10 mg/day. Subjects
were randomly assigned to either 10 mg/day or 80 mg/day of LIPITOR and followed
for a median duration of 4.9 years. The primary endpoint was the time-to-first
occurrence of any of the following major cardiovascular events (MCVE): death due
to CHD, non-fatal myocardial infarction, resuscitated cardiac arrest, and fatal
and non-fatal stroke. The mean LDL-C, TC, TG, non-HDL, and HDL cholesterol
levels at 12 weeks were 73, 145, 128, 98, and 47 mg/dL during treatment with 80
mg of LIPITOR and 99, 177, 152, 129, and 48 mg/dL during treatment with 10 mg of
LIPITOR.
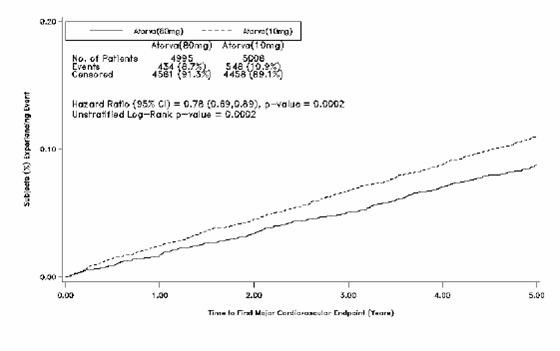
Treatment with LIPITOR 80 mg/day significantly reduced the rate of MCVE (434
events in the 80mg/day group vs. 548 events in the 10 mg/day group) with a
relative risk reduction of 22%, HR 0.78, 95% CI (0.69,0.89), p=0.0002 (see Figure5 and Table 5). The overall risk
reduction was consistent regardless of age (less than 65, greate than or equal to 65) or gender.
Figure 5. Effect of LIPITOR 80 mg/day vs. 10 mg/day on Time to
Occurrence ofMajor Cardiovascular Events (TNT)
Suicide, homicide and other traumatic non-CV death
9
(0.2)
15
(0.3)
1.67 (0.73, 3.82)
HR=hazard ratio, CHD =coronary heart disease; CI=confidence interval; MI=myocardial infarction;
CHF=congestive heart failure; CV=cardiovascular; PVD=peripheral vascular disease; CABG=coronary artery bypass
graftConfidence intervals for the Secondary Endpoints were not adjusted for multiple
comparisons.
*Â Â Â Â Atorvastatin 80 mg: atorvastatin 10 mg
†    Secondary endpoints not included in primary endpoint
‡    Component of other secondary endpoints
Of the events that comprised the primary efficacy endpoint, treatment with
LIPITOR 80 mg/day significantly reduced the rate of non-fatal, non-procedure
related MI and fatal and non-fatal stroke, but not CHD death or resuscitated
cardiac arrest (Table 5). Of the predefined secondary
endpoints, treatment with LIPITOR 80 mg/day significantly reduced the rate of
coronary revascularization, angina, and hospitalization for heart failure, but
not peripheral vascular disease. The reduction in the rate of CHF with
hospitalization was only observed in the 8% of patients with a prior history of
CHF.
There was no significant difference between the treatment groups for
all-cause mortality (Table 5). The proportions of subjects
who experienced cardiovascular death, including the components of CHD death and
fatal stroke, were numerically smaller in the LIPITOR 80 mg group than in the
LIPITOR 10 mg treatment group. The proportions of subjects who experienced
noncardiovascular death were numerically larger in the LIPITOR 80 mg group than
in the LIPITOR 10 mg treatment group.
In the Incremental Decrease in Endpoints Through Aggressive Lipid Lowering
Study (IDEAL), treatment with LIPITOR 80 mg/day was compared to treatment with
simvastatin 20–40 mg/day in 8,888 subjects up to 80 years of age with a history
of CHD to assess whether reduction in CV risk could be achieved. Patients were
mainly male (81%), white (99%) with an average age of 61.7 years, and an average
LDL-C of 121.5 mg/dL at randomization; 76% were on statin therapy. In this
prospective, randomized, open-label, blinded endpoint (PROBE) trial with no
run-in period, subjects were followed for a median duration of 4.8 years. The
mean LDL-C, TC, TG, HDL, and non-HDL cholesterol levels at Week 12 were 78, 145,
115, 45, and 100 mg/dL during treatment with 80 mg of LIPITOR and 105, 179, 142,
47, and 132 mg/dL during treatment with 20–40 mg of simvastatin.
There was no significant difference between the treatment groups for the
primary endpoint, the rate of first major coronary event (fatal CHD, nonfatal MI
and resuscitated cardiac arrest): 411 (9.3%) in the LIPITOR 80 mg/day group vs.
463 (10.4%) in the simvastatin 20–40 mg/day group, HR 0.89, 95% CI ( 0.78,
1.01), p=0.07.
There were no significant differences between the treatment groups for
all-cause mortality: 366 (8.2%) in the LIPITOR 80 mg/day group vs. 374 (8.4%) in
the simvastatin 20–40 mg/day group. The proportions of subjects who experienced
CV or non-CV death were similar for the LIPITOR 80 mg group and the simvastatin
20–40 mg group. Atorvastatin Studies in Hyperlipidemia (Heterozygous
Familial and Nonfamilial) and Mixed Dyslipidemia (Fredrickson Types IIa and
IIb) Atorvastatin reduces total-C, LDL-C, VLDL-C, apo B, and TG, and
increases HDL-C in patients with hyperlipidemia and mixed dyslipidemia.
Therapeutic response is seen within 2 weeks, and maximum response is usually
achieved within 4 weeks and maintained during chronic therapy.
Atorvastatin is effective in a wide variety of patient populations with
hyperlipidemia, with and without hypertriglyceridemia, in men and women, and in
the elderly.
In two multicenter, placebo-controlled, dose-response studies in patients
with hyperlipidemia, atorvastatin given as a single dose over 6 weeks,
significantly reduced total-C, LDL-C, apo B, and TG (pooled results are provided
in Table 6).
Table 6. Dose-Response in Patients With Primary Hyperlipidemia (Adjusted Mean Percent Change From Baseline)*
Dose
NÂ Â Â Â Â
TC
LDL-C
Apo B
TG
HDL-C
Non-HDL-C/ HDL-C
Placebo   Â
21Â Â Â Â Â
4
4
3
10
-3
7
10
22Â Â Â Â Â
-29
-39
-32
-19
6
-34
20
20Â Â Â Â Â
-33
-43
-35
-26
9
-41
40
21Â Â Â Â
-37
-50
-42
-29
6
-45
80
23Â Â Â Â Â
-45
-60
-50
-37
5
-53
*Â Â Â Â Results are pooled from 2 dose-response studies.
In patients with Fredrickson Types IIa and IIb
hyperlipoproteinemia pooled from 24 controlled trials, the median (25th and 75th percentile) percent changes
from baseline in HDL-C for atorvastatin 10, 20, 40, and 80 mg were 6.4 (-1.4,
14), 8.7 (0, 17), 7.8 (0, 16), and 5.1 (-2.7, 15), respectively. Additionally,
analysis of the pooled data demonstrated consistent and significant decreases in
total-C, LDL-C, TG, total-C/HDL-C, and LDL-C/HDL-C.
In three multicenter, double-blind studies in patients with hyperlipidemia,
atorvastatin was compared to other statins. After randomization, patients were
treated for 16 weeks with either atorvastatin 10 mg per day or a fixed dose of
the comparative agent (Table 7).
Table 7. Mean Percent Change From Baseline at Endpoint (Double-Blind, Randomized, Active-Controlled Trials)
*Â Â Â Â Significantly different from lovastatin, ANCOVA, p less than or equal to 0.05
†    A negative value for the 95% CI for the difference between treatments favors
atorvastatin for all except HDL-C, for which a positive value favors
atorvastatin. If the range does not include 0, this indicates a statistically
significant difference.
‡    Significantly different from pravastatin, ANCOVA, p less than or equal to 0.05
§      Significantly different from simvastatin, ANCOVA, p less than or equal to 0.05
The impact on clinical outcomes of the differences in lipid-altering effects
between treatments shown in Table 7 is not known. Table 7 does not contain data
comparing the effects of atorvastatin 10 mg and higher doses of lovastatin,
pravastatin, and simvastatin. The drugs compared in the studies summarized in
the table are not necessarily interchangeable. Atorvastatin Effects in Hypertriglyceridemia
(Fredrickson Type IV) The response to atorvastatin in 64 patients with isolated
hypertriglyceridemia treated across several clinical trials is shown in the
table below (Table 8). For the atorvastatin-treated patients, median (min, max)
baseline TG level was 565 (267–1502).
Table 8. Combined Patients With Isolated Elevated TG: Median (min, max)
Percent Changes From Baseline
Placebo(N=12)
Atorvastatin 10 mg(N=37)
Atorvastatin 20 mg(N=13)
Atorvastatin 80 mg(N=14)
Triglycerides
-12.4 (-36.6, 82.7)
-41.0 (-76.2, 49.4)
-38.7 (-62.7, 29.5)
-51.8 (-82.8, 41.3)
Total-C
-2.3 (-15.5, 24.4)
-28.2 (-44.9, -6.8)
-34.9 (-49.6, -15.2)
-44.4 (-63.5, -3.8)
LDL-C
3.6 (-31.3, 31.6)
-26.5 (-57.7, 9.8)
-30.4 (-53.9, 0.3)
-40.5 (-60.6, -13.8)
HDL-C
3.8 (-18.6, 13.4)
13.8 (-9.7, 61.5)
11.0 (-3.2, 25.2)
7.5 (-10.8, 37.2)
VLDL-C
-1.0 (-31.9, 53.2)
-48.8 (-85.8, 57.3)
-44.6 (-62.2, -10.8)
-62.0 (-88.2, 37.6)
non-HDL-C
-2.8 (-17.6, 30.0)
-33.0 (-52.1, -13.3)
-42.7 (-53.7, -17.4)
-51.5 (-72.9, -4.3)
Atorvastatin Effects in Dysbetalipoproteinemia
(Fredrickson Type III) The results of an open-label crossover study of atorvastatin in
16 patients (genotypes: 14 apo E2/E2 and 2 apo E3/E2) with
dysbetalipoproteinemia (Fredrickson Type III) are
shown in the table below (Table 9).
Table 9. Open-Label Crossover Study of 16 Patients With
Dysbetalipoproteinemia (Fredrickson Type III)
Median % Change (min, max)
Median (min, max) atBaseline (mg/dL)
Atorvastatin 10 mg
Atorvastatin 80 mg
Total-C
442 (225, 1320)
-37 (-85, 17)
-58 (-90, -31)
Triglycerides
678 (273, 5990)
-39 (-92, -8)
-53 (-95, -30)
IDL-C + VLDL-C
215 (111, 613)
-32 (-76, 9)
-63 (-90, -8)
non-HDL-C
411 (218, 1272)
-43 (-87, -19)
-64 (-92, -36)
Atorvastatin Effects in Homozygous Familial
Hypercholesterolemia In a study without a concurrent control group, 29 patients ages 6
to 37 years with homozygous FH received maximum daily doses of 20 to 80 mg of
atorvastatin. The mean LDL-C reduction in this study was 18%. Twenty-five
patients with a reduction in LDL-C had a mean response of 20% (range of 7% to
53%, median of 24%); the remaining 4 patients had 7% to 24% increases in LDL-C.
Five of the 29 patients had absent LDL-receptor function. Of these, 2 patients
also had a portacaval shunt and had no significant reduction in LDL-C. The
remaining 3 receptor-negative patients had a mean LDL-C reduction of 22%. Atorvastatin Effects in Heterozygous Familial
Hypercholesterolemic Pediatric Patients In a double-blind, placebo-controlled study followed by an
open-label phase, 187 boys and postmenarchal girls 10–17 years of age (mean age
14.1 years) with heterozygous FH or severe hypercholesterolemia, were randomized
to atorvastatin (n=140) or placebo (n=47) for 26 weeks and then all received
atorvastatin for 26 weeks. Inclusion in the study required 1) a baseline LDL-C
level ≥ 190 mg/dL or 2) a baseline LDL-C level ≥ 160 mg/dL and positive family
history of FH or documented premature cardiovascular disease in a first- or
second-degree relative. The mean baseline LDL-C value was 218.6 mg/dL (range:
138.5–385.0 mg/dL) in the atorvastatin group compared to 230.0 mg/dL (range:
160.0–324.5 mg/dL) in placebo group. The dosage of atorvastatin (once daily) was
10 mg for the first 4 weeks and up-titrated to 20 mg if the LDL-C level was >
130 mg/dL. The number of atorvastatin-treated patients who required up-titration
to 20 mg after Week 4 during the double-blind phase was 80 (57.1%).
Atorvastatin significantly decreased plasma levels of total-C, LDL-C,
triglycerides, and apolipoprotein B during the 26 week double-blind phase (see
Table 10).
Table 10. Lipid-altering Effects of Atorvastatin in Adolescent Boys and
Girls with Heterozygous Familial Hypercholesterolemia or Severe
Hypercholesterolemia (Mean Percent Change From Baseline at Endpoint in
Intention-to-Treat Population)
DOSAGE
N
Total-C
LDL-C
HDL-C
TG
Apolipoprotein B
Placebo
47
-1.5
-0.4
-1.9
1.0
0.7
Atorvastatin
140
-31.4
-39.6
2.8
-12.0
-34.0
The mean achieved LDL-C value was 130.7 mg/dL (range: 70.0–242.0 mg/dL) in
the atorvastatin group compared to 228.5 mg/dL (range: 152.0–385.0 mg/dL) in the
placebo group during the 26 week double-blind phase.
The safety and efficacy of atorvastatin doses above 20 mg have not been
studied in controlled trials in children. The long-term efficacy of atorvastatin
therapy in childhood to reduce morbidity and mortality in adulthood has not been
established. Clinical Study of Combined Amlodipine and
Atorvastatin in Patients with Hypertension and Dyslipidemia In a double-blind, placebo-controlled study, a total of 1660
patients with co-morbid hypertension and dyslipidemia received once daily
treatment with eight dose combinations of amlodipine and atorvastatin (5/10,
10/10, 5/20, 10/20, 5/40, 10/40, 5/80, or 10/80 mg), amlodipine alone (5 mg or
10 mg), atorvastatin alone (10 mg, 20 mg, 40 mg, or 80 mg) or placebo. In addition to concomitant hypertension and dyslipidemia,
15% of the patients had diabetes mellitus, 22% were smokers and 14% had a
positive family history of cardiovascular disease. At eight weeks, all eight
combination-treatment groups of amlodipine and atorvastatin demonstrated
statistically significant dose-related reductions in systolic blood pressure
(SBP), diastolic blood pressure (DBP) and LDL-C compared to placebo, with no
overall modification of effect of either component on SBP, DBP and LDL-C (Table 11).
Table 11. Efficacy in Terms of Reduction in Blood Pressure and
LDL-C
Efficacy of the Combined Treatments in
Reducing Systolic BP
Parameter / Analysis
ATO 0 mg
ATO 10 mg
ATO 20 mg
ATO 40 mg
ATO 80 mg
Mean change(mmHg)
-3.0
-4.5
-6.2
-6.2
-6.4
AML 0 mg
Difference versusplacebo (mmHg)
-
-1.5
-3.2
-3.2
-3.4
Mean change(mmHg)
-12.8
-13.7
-15.3
-12.7
-12.2
AML 5 mg
Difference versusplacebo (mmHg)
-9.8
-10.7
-12.3
-9.7
-9.2
Mean change(mmHg)
-16.2
-15.9
-16.1
-16.3
-17.6
AML 10 mg
Difference versusplacebo (mmHg)
-13.2
-12.9
-13.1
-13.3
-14.6
Efficacy of the Combined Treatments in Reducing
Diastolic BP
Parameter / Analysis
ATO 0 mg
ATO 10 mg
ATO 20 mg
ATO 40 mg
ATO 80 mg
Mean change(mmHg)
-3.3
-4.1
-3.9
-5.1
-4.1
AML 0 mg
Difference versusplacebo (mmHg)
-
-0.8
-0.6
-1.8
-0.8
Mean change(mmHg)
-7.6
-8.2
-9.4
-7.3
-8.4
AML 5 mg
Difference versusplacebo (mmHg)
-4.3
-4.9
-6.1
-4.0
-5.1
Mean change(mmHg)
-10.4
-9.1
-10.6
-9.8
-11.1
AML 10 mg
Difference versusplacebo (mmHg)
-7.1
-5.8
-7.3
-6.5
-7.8
Efficacy of the Combined Treatments in Reducing LDL-C
(% change)
Parameter / Analysis
ATO 0 mg
ATO 10 mg
ATO 20 mg
ATO 40 mg
ATO 80 mg
AML 0 mg
Mean % change
-1.1
-33.4
-39.5
-43.1
-47.2
AML 5 mg
Mean % change
-0.1
-38.7
-42.3
-44.9
-48.4
AML 10 mg
Mean % change
-2.5
-36.6
-38.6
-43.2
-49.1
Indications And Usage
CADUET (amlodipine and atorvastatin) is indicated in patients for
whom treatment with both amlodipine and atorvastatin is appropriate. Amlodipine1.
Hypertension
:
Amlodipine is indicated for the treatment of hypertension. It may be used alone
or in combination with other antihypertensive agents;
2.
Coronary Artery Disease (CAD)
Chronic Stable Angina: Amlodipine is indicated for the
treatment of chronic stable angina. Amlodipine may be used alone or in
combination with other antianginal or antihypertensive agents;
Vasospastic Angina (Prinzmetal's or Variant Angina):
Amlodipine is indicated for the treatment of confirmed or suspected vasospastic
angina. Amlodipine may be used as monotherapy or in combination with other
antianginal drugs.
Angiographically Documented
CAD: In patients with recently documented CAD by angiography and without
heart failure or an ejection fraction less than 40%, amlodipine is indicated to reduce
the risk of hospitalization due to angina and to reduce the risk of a coronary
revascularization procedure. AND Atorvastatin Therapy with lipid-altering agents should be only one component
of multiple risk factor intervention in individuals at significantly increased
risk for atherosclerotic vascular disease due to hypercholesterolemia. Drug
therapy is recommended as an adjunct to diet when the response to a diet
restricted in saturated fat and cholesterol and other nonpharmacologic measures
alone has been inadequate. In patients with CHD or multiple risk factors for
CHD, the atorvastatin component of CADUET can be started simultaneously with
diet restriction. 1.
Prevention of Cardiovascular Disease: In
adult patients without clinically evident coronary heart disease, but with
multiple risk factors for coronary heart disease such as age, smoking,
hypertension, low HDL-C, or a family history of early coronary heart disease,
atorvastatin is indicated to:
Reduce the risk of myocardial infarction
Reduce the risk of stroke
Reduce the risk for revascularization procedures and angina
In
patients with type 2 diabetes, and without clinically evident coronary heart
disease, but with multiple risk factors for coronary heart disease such as
retinopathy, albuminuria, smoking, or hypertension, LIPITOR is indicated to:
Reduce the risk of myocardial infarction
Reduce the risk of stroke;
In patients with clinically evident
coronary heart disease, LIPITOR is indicated to:
Reduce the risk of non-fatal myocardial infarction
Reduce the risk of fatal and non-fatal stroke
Reduce the risk for revascularization procedures
Reduce the risk of hospitalization for CHF
Reduce the risk of angina
2.
Heterozygous Familial and Nonfamilial
Hyperlipidemia
: Atorvastatin is indicated as an
adjunct to diet to reduce elevated total-C, LDL-C, apo B, and TG levels and to
increase HDL-C in patients with primary hypercholesterolemia (heterozygous
familial and nonfamilial) and mixed dyslipidemia (Fredrickson Types IIa and IIb);
3.
Elevated Serum TG Levels
: Atorvastatin is indicated as an adjunct to diet for the
treatment of patients with elevated serum TG levels (Fredrickson Type IV);
4.
Primary Dysbetalipoproteinemia
: Atorvastatin is indicated for the treatment of patients with
primary dysbetalipoproteinemia (Fredrickson Type III)
who do not respond adequately to diet;
5.
Homozygous Familial Hypercholesterolemia
: Atorvastatin is indicated to reduce total-C and LDL-C in
patients with homozygous familial hypercholesterolemia as an adjunct to other
lipid-lowering treatments (e.g., LDL apheresis) or if such treatments are
unavailable;
6.
Pediatric Patients
:
Atorvastatin is indicated as an adjunct to diet to reduce total-C, LDL-C, and
apo B levels in boys and postmenarchal girls, 10 to 17 years of age, with
heterozygous familial hypercholesterolemia if after an adequate trial of diet
therapy the following findings are present:
LDL-C remains greater than or equal to 190 mg/dL or
LDL-C remains greater than or equal to 160 mg/dL and:
there is a positive family history of premature cardiovascular disease or
two or more other CVD risk factors are present in the pediatric patients.
The antidyslipidemic component of CADUET has not been studied in conditions
where the major lipoprotein abnormality is elevation of chylomicrons (Fredrickson Types I and V).
Contraindications
CADUET contains atorvastatin and is therefore contraindicated in
patients with active liver disease, which may include unexplained persistent
elevations in hepatic transaminase levels.
CADUET is contraindicated in patients with known hypersensitivity to any
component of this medication. Pregnancy and Lactation CADUET contains atorvastatin and is therefore contraindicated in
women who are pregnant or may become pregnant. The atorvastatin component of
CADUET may cause fetal harm when administered to a pregnant woman. Serum
cholesterol and triglycerides increase during normal pregnancy, and cholesterol
or cholesterol derivatives are essential for fetal development. Atherosclerosis
is a chronic process and discontinuation of lipid-lowering drugs during
pregnancy should have little impact on the outcome of long-term therapy of
primary hypercholesterolemia.
There are no adequate and well-controlled studies of atorvastatin use during
pregnancy; however in rare reports congenital anomalies were observed following
intrauterine exposure to statins. In rat and rabbit animal reproduction studies,
atorvastatin revealed no evidence of teratogenicity. CADUET, WHICH INCLUDES
ATORVASTATIN, SHOULD BE ADMINISTERED TO WOMEN OF CHILDBEARING AGE ONLY WHEN SUCH
PATIENTS ARE HIGHLY UNLIKELY TO CONCEIVE AND HAVE BEEN INFORMED OF THE POTENTIAL
HAZARDS. If the patient becomes pregnant while taking this drug, therapy should
be discontinued immediately and the patient apprised of the potential hazard to
the fetus (see PRECAUTIONS,
Pregnancy).
It is not known whether atorvastatin or amlodipine are excreted into human
milk; however a small amount of another statin does pass into breast milk.
Because statins have the potential for serious adverse reactions in nursing
infants, women taking CADUET should not breastfeed their infants (see PRECAUTIONS, Nursing
Mothers).
Warnings
Skeletal Muscle Rare cases of rhabdomyolysis with acute renal
failure secondary to myoglobinuria have been reported with the atorvastatin
component of CADUET and with other statins. A history of renal impairment
may be a risk factor for the development of rhabdomyolysis. Such patients merit
closer monitoring for skeletal muscle effects.
The atorvastatin component of CADUET, like other statins, occasionally causes
myopathy, defined as muscle aches or muscle weakness in conjunction with
increases in creatine phosphokinase (CPK) values >10 times ULN. The
concomitant use of higher doses of atorvastatin with certain drugs such as
cyclosporine and strong CYP3A4 inhibitors (e.g., clarithromycin, itraconazole
and HIV protease inhibitors) increases the risk of myopathy/rhabdomyolysis.
Myopathy should be considered in any patient with diffuse myalgias, muscle
tenderness or weakness, or marked elevation of CPK. Patients should be advised
to report promptly unexplained muscle pain, tenderness or weakness, particularly
if accompanied by malaise or fever. CADUET therapy should be discontinued if
markedly elevated CPK levels occur or myopathy is diagnosed or suspected.
The risk of myopathy during treatment with statins is increased with
concurrent administration of cyclosporine, fibric acid derivatives,
erythromycin, clarithromycin, combination of ritonavir plus saquinavir or
lopinavir plus ritonavir, niacin, or azole antifungals. Physicians considering
combined therapy with CADUET and fibric acid derivatives, erythromycin,
clarithromycin, a combination of ritonavir plus saquinavir or lopinavir plus
ritonavir, immunosuppressive drugs, azole antifungals, or lipid-modifying doses
of niacin should carefully weigh the potential benefits and risks and should
carefully monitor patients for any signs or symptoms of muscle pain, tenderness,
or weakness, particularly during the initial months of therapy and during any
periods of upward dosage titration of either drug. Lower starting and
maintenance doses of atorvastatin should be considered when taken concomitantly
with the aforementioned drugs (see PRECAUTIONS, Drug
Interactions). Periodic creatine phosphokinase (CPK) determinations
may be considered in such situations, but there is no assurance that such
monitoring will prevent the occurrence of severe myopathy.
TABLE 12 Atorvastatin Drug Interactions Associated with Increased Risk
of Myopathy/Rhabdomyolysis
Interacting Agents
Prescribing Recommendations
Cyclosporine
Do not exceed 10 mg atorvastatin daily
Clarithromycin, Itraconazole, HIV protease inhibitors
(ritonavir plus saquinavir or lopinavir plus ritonavir,)
Caution when exceeding doses > 20mg atorvastatin daily. The
lowest dose necessary should be used.
In patients taking CADUET, therapy should be temporarily
withheld or discontinued in any patient with an acute, serious condition
suggestive of a myopathy or having a risk factor predisposing to the development
of renal failure secondary to rhabdomyolysis (e.g., severe acute infection,
hypotension, major surgery, trauma, severe metabolic, endocrine and electrolyte
disorders, and uncontrolled seizures). Liver Dysfunction Statins, like the atorvastatin component of CADUET and like some
other lipid-lowering therapies, have been associated with biochemical
abnormalities of liver function. Persistent elevations (>3
times the upper limit of normal [ULN] occurring on 2 or more occasions) in serum
transaminases occurred in 0.7% of patients who received atorvastatin in clinical
trials. The incidence of these abnormalities was 0.2%, 0.2%, 0.6%, and 2.3% for
10, 20, 40, and 80 mg, respectively.
In clinical trials in patients taking the atorvastatin component of CADUET,
the following has been observed. One patient in clinical trials developed
jaundice. Increases in liver function tests (LFT) in other patients were not
associated with jaundice or other clinical signs or symptoms. Upon dose
reduction, drug interruption, or discontinuation, transaminase levels returned
to or near pretreatment levels without sequelae. Eighteen of 30 patients, with
persistent LFT elevations continued treatment with a reduced dose of
atorvastatin.
It is recommended that liver function tests be performed prior to and at 12
weeks following both the initiation of therapy and any elevation of dose, and
periodically (e.g., semiannually) thereafter. Liver enzyme changes generally
occur in the first 3 months of treatment with the atorvastatin component of
CADUET. Patients who develop increased transaminase levels should be monitored
until the abnormalities resolve. Should an increase in ALT or AST of >3 times
ULN persist, reduction of dose or withdrawal of CADUET is recommended.
Active liver disease or unexplained persistent transaminase elevations are
contraindications to the use of CADUET (see CONTRAINDICATIONS). Increased Angina and/or Myocardial Infarction Worsening angina and acute myocardial infarction can develop
after starting or increasing the dose of amlodipine, particularly in patients
with severe obstructive coronary artery disease.
Precautions
Hypotension Symptomatic hypotension is possible, particularly in patients
with severe aortic stenosis. Because of the gradual onset of action, acute
hypotension is unlikely. Beta-Blocker Withdrawal The amlodipine component of CADUET is not a beta-blocker and
therefore gives no protection against the dangers of abrupt beta-blocker
withdrawal; any such withdrawal should be by gradual reduction of the dose of
beta-blocker. Endocrine Function Statins, such as the atorvastatin component of CADUET interfere
with cholesterol synthesis and theoretically might blunt adrenal and/or gonadal
steroid production. Clinical studies have shown that atorvastatin does not
reduce basal plasma cortisol concentration or impair adrenal reserve. The
effects of statins on male fertility have not been studied in adequate numbers
of patients. The effects, if any, on the pituitary-gonadal axis in premenopausal
women are unknown. Use caution when administering a statin with drugs that may
decrease the levels or activity of endogenous steroid hormones, such as
ketoconazole, spironolactone, and cimetidine. CNS ToxicityStudies with atorvastatin Brain hemorrhage was seen in a female dog treated with
atorvastatin calcium for 3 months at a dose equivalent to 120 mg
atorvastatin/kg/day. Brain hemorrhage and optic nerve vacuolation were seen in
another female dog that was sacrificed in moribund condition after 11 weeks of
escalating doses of atorvastatin calcium equivalent to up to 280 mg
atorvastatin/kg/day. The 120 mg/kg dose of atorvastatin resulted in a systemic
exposure approximately 16 times the human plasma area-under-the-curve (AUC, 0–24
hours) based on the maximum human dose of 80 mg/day. A single tonic convulsion
was seen in each of 2 male dogs (one treated with atorvastatin calcium at a dose
equivalent to 10 mg atorvastatin/kg/day and one at a dose equivalent to 120 mg
atorvastatin/kg/day) in a 2-year study. No CNS lesions have been observed in
mice after chronic treatment for up to 2 years at doses of atorvastatin calcium
equivalent to up to 400 mg atorvastatin/kg/day or in rats at doses equivalent to
up to 100 mg atorvastatin/kg/day. These doses were 6 to 11 times (mouse) and 8
to 16 times (rat) the human AUC (0–24) based on the maximum recommended human
dose of 80 mg atorvastatin/day.
CNS vascular lesions, characterized by perivascular hemorrhages, edema, and
mononuclear cell infiltration of perivascular spaces, have been observed in dogs
treated with other statins. A chemically similar drug in this class produced
optic nerve degeneration (Wallerian degeneration of retinogeniculate fibers) in
clinically normal dogs in a dose-dependent fashion at a dose that produced
plasma drug levels about 30 times higher than the mean drug level in humans
taking the highest recommended dose. Use in Patients with Recent Stroke or TIAStudies with atorvastatin In a post-hoc analysis of the Stroke Prevention by Aggressive
Reduction in Cholesterol Levels (SPARCL) study where atorvastatin 80 mg vs.
placebo was administered in 4,731 subjects without CHD who had a stroke or TIA
within the preceding 6 months, a higher incidence of hemorrhagic stroke was seen
in the atorvastatin 80 mg group compared to placebo (55, 2.3% atorvastatin vs.
33, 1.4% placebo; HR: 1.68, 95% CI: 1.09, 2.59; p=0.0168). The incidence of
fatal hemorrhagic stroke was similar across treatment groups (17 vs. 18 for the
atorvastatin and placebo groups, respectively). The incidence of nonfatal
hemorrhagic stroke was significantly higher in the atorvastatin group (38, 1.6%)
as compared to the placebo group (16, 0.7%). Some baseline characteristics,
including hemorrhagic and lacunar stroke on study entry, were associated with a
higher incidence of hemorrhagic stroke in the atorvastatin group (see ADVERSE REACTIONS, The Atorvastatin Component of
CADUET). Information for Patients Because of the risk of myopathy with statins, the drug class to
which the atorvastatin component of CADUET belongs, advise patients to promptly
report unexplained muscle pain, tenderness, or weakness, particularly if
accompanied by malaise or fever. Drug Interactions Data from a drug-drug interaction study involving 10 mg of
amlodipine and 80 mg of atorvastatin in healthy subjects indicate that the
pharmacokinetics of amlodipine are not altered when the drugs are
coadministered. The effect of amlodipine on the pharmacokinetics of atorvastatin
showed no effect on the Cmax: 91% (90% confidence interval: 80 to 103%), but the
AUC of atorvastatin increased by 18% (90% confidence interval: 109 to 127%) in
the presence of amlodipine, which was not clinically meaningful.
No drug interaction studies have been conducted with CADUET and other drugs,
although studies have been conducted in the individual amlodipine and
atorvastatin components, as described below: Studies with Amlodipine In vitro data in human plasma indicate
that amlodipine has no effect on the protein binding of drugs tested (digoxin,
phenytoin, warfarin, and indomethacin).
Cimetidine: Co-administration of amlodipine with
cimetidine did not alter the pharmacokinetics of amlodipine.
Maalox® (antacid): Co-administration of the antacid
Maalox with a single dose of amlodipine had no significant effect on the
pharmacokinetics of amlodipine.
Sildenafil: A single 100 mg dose of sildenafil
(Viagra®) in subjects with essential hypertension had no effect on the
pharmacokinetic parameters of amlodipine. When amlodipine and sildenafil were
used in combination, each agent independently exerted its own blood pressure
lowering effect.
Digoxin: Co-administration of amlodipine with digoxin
did not change serum digoxin levels or digoxin renal clearance in normal
volunteers.
Ethanol (alcohol): Single and multiple 10 mg doses of
amlodipine had no significant effect on the pharmacokinetics of ethanol.
Warfarin: Co-administration of amlodipine with
warfarin did not change the warfarin prothrombin response time.
In clinical trials, amlodipine has been safely administered with thiazide
diuretics, beta-blockers, angiotensin-converting enzyme inhibitors, long-acting
nitrates, sublingual nitroglycerin, digoxin, warfarin, non-steroidal
anti-inflammatory drugs, antibiotics, and oral hypoglycemic drugs. Studies with Atorvastatin The risk of myopathy during treatment with statins is increased
with concurrent administration of fibric acid derivatives, lipid-modifying doses
of niacin, cyclosporine, or strong CYP 3A4 inhibitors (e.g., clarithromycin, HIV
protease inhibitors, and itraconazole) (see WARNINGS, Skeletal Muscle, and CLINICAL
PHARMACOLOGY). Strong Inhibitors of CYP 3A4:
Atorvastatin is metabolized by cytochrome P450 3A4. Concomitant administration
of atorvastatin with strong inhibitors of CYP 3A4 can lead to increases in
plasma concentrations of atorvastatin. The extent of interaction and
potentiation of effects depends on the variability of effect on CYP 3A4. Â
Clarithromycin: Atorvastatin AUC was significantly
increased with concomitant administration of atorvastatin 80 mg with
clarithromycin (500 mg twice daily) compared to that of atorvastatin alone (see
CLINICAL
PHARMACOLOGY). Therefore, in patients taking clarithromycin, use
caution when administering atorvastatin doses > 20 mg (see WARNINGS, Skeletal Muscle,
and DOSAGE AND
ADMINISTRATION).
Â
Combination of Protease Inhibitors: Atorvastatin AUC
was significantly increased with concomitant administration of atorvastatin 40
mg with ritonavir plus saquinavir (400 mg twice daily) or atorvastatin 20 mg
with lopinavir plus ritonavir (400 mg + 100 mg twice daily) compared to that of
atorvastatin alone (see CLINICAL PHARMACOLOGY). Therefore, in
patients taking HIV protease inhibitors, use caution when administering
atorvastatin doses ≥20 mg (see WARNINGS, Skeletal Muscle, and DOSAGE AND
ADMINISTRATION).
Â
Itraconazole: Atorvastatin AUC was significantly
increased with concomitant administration of atorvastatin 40 mg and itraconazole
200 mg (see CLINICAL
PHARMACOLOGY). Therefore, in patients taking itraconazole, use
caution when administering atorvastatin doses ≥20 mg (see WARNINGS, Skeletal Muscle, and DOSAGE AND
ADMINISTRATION). Grapefruit juice: Contains one or more
components that inhibit CYP 3A4 and can increase plasma concentrations of
atorvastatin, especially with excessive grapefruit juice consumption (>1.2
liters per day). Cyclosporine: Atorvastatin and
atorvastatin-metabolites are substrates of the OATP1B1 transporter. Inhibitors
of the OATP1B1 (e.g., cyclosporine) can increase the bioavailability of
atorvastatin. Atorvastatin AUC was significantly increased with concomitant
administration of atorvastatin 10 mg and cyclosporine 5.2 mg/kg/day compared to
that of atorvastatin alone (see CLINICAL PHARMACOLOGY). In cases where
coadministration of atorvastatin with cyclosporine is necessary, the dose of
atorvastatin should not exceed 10 mg (see WARNINGS, Skeletal Muscle). Rifampin or other Inducers of Cytochrome P450
3A4: Concomitant administration of atorvastatin with inducers of
cytochrome P450 3A4 (e.g., efavirenz, rifampin) can lead to variable reductions
in plasma concentrations of atorvastatin. Due to the dual interaction mechanism
of rifampin, simultaneous co-administration of atorvastatin with rifampin is
recommended, as delayed administration of atorvastatin after administration of
rifampin has been associated with a significant reduction in atorvastatin plasma
concentrations.
Digoxin: When multiple doses of atorvastatin and
digoxin were coadministered, steady-state plasma digoxin concentrations
increased by approximately 20%. Patients taking digoxin should be monitored
appropriately.
Oral Contraceptives: Coadministration of atorvastatin
and an oral contraceptive increased AUC values for norethindrone and ethinyl
estradiol (see CLINICAL
PHARMACOLOGY). These increases should be considered when selecting an
oral contraceptive for a woman taking CADUET.
Warfarin: Atorvastatin had no clinically significant
effect on prothrombin time when administered to patients receiving chronic
warfarin treatment. Drug/Laboratory Test Interactions None known. Carcinogenesis, Mutagenesis, Impairment of
FertilityStudies with amlodipine Rats and mice treated with amlodipine maleate in the diet for up
to two years, at concentrations calculated to provide daily dosage levels of
0.5, 1.25, and 2.5 mg amlodipine/kg/day, showed no evidence of a carcinogenic
effect of the drug. For the mouse, the highest dose was, on a mg/m2 basis, similar to the maximum recommended human dose of 10 mg
amlodipine/day1.
For the rat, the highest dose level was, on a mg/m2
basis, about twice the maximum recommended human dose1.
Mutagenicity studies conducted with amlodipine maleate revealed no drug
related effects at either the gene or chromosome levels.
There was no effect on the fertility of rats treated orally with amlodipine
maleate (males for 64 days and females for 14 days prior to mating) at doses up
to 10 mg amlodipine/kg/day (8 times1 the
maximum recommended human dose of 10 mg/day on a mg/m2
basis). 1Based on patent weight of 50 kg. Studies with atorvastatin In a 2-year carcinogenicity study with atorvastatin calcium in
rats at dose levels equivalent to 10, 30, and 100 mg atorvastatin/kg/day, 2 rare
tumors were found in muscle in high-dose females: in one, there was a
rhabdomyosarcoma and, in another, there was a fibrosarcoma. This dose represents
a plasma AUC (0–24) value of approximately 16 times the mean human plasma drug
exposure after an 80 mg oral dose.
A 2-year carcinogenicity study in mice given atorvastatin calcium at dose
levels equivalent to 100, 200, and 400 mg atorvastatin/kg/day resulted in a
significant increase in liver adenomas in high-dose males and liver carcinomas
in high-dose females. These findings occurred at plasma AUC (0–24) values of
approximately 6 times the mean human plasma drug exposure after an 80 mg oral
dose.
In vitro, atorvastatin was not mutagenic or
clastogenic in the following tests with and without metabolic activation: the
Ames test with Salmonella typhimurium and Escherichia coli, the HGPRT forward mutation assay in
Chinese hamster lung cells, and the chromosomal aberration assay in Chinese
hamster lung cells. Atorvastatin was negative in the in
vivo mouse micronucleus test.
There were no effects on fertility when rats were given atorvastatin calcium
at doses equivalent to up to 175 mg atorvastatin/kg/day (15 times the human
exposure). There was aplasia and aspermia in the epididymides of 2 of 10 rats
treated with atorvastatin calcium at a dose equivalent to 100 mg
atorvastatin/kg/day for 3 months (16 times the human AUC at the 80 mg dose);
testis weights were significantly lower at 30 and 100 mg/kg/day and epididymal
weight was lower at 100 mg/kg/day. Male rats given the equivalent of 100 mg
atorvastatin/kg/day for 11 weeks prior to mating had decreased sperm motility,
spermatid head concentration, and increased abnormal sperm. Atorvastatin caused
no adverse effects on semen parameters, or reproductive organ histopathology in
dogs given doses of atorvastatin calcium equivalent to 10, 40, or 120 mg
atorvastatin/kg/day for two years. PregnancyPregnancy Category X (see CONTRAINDICATIONS)
CADUET contains atorvastatin and is therefore contraindicated in women who
are pregnant or may become pregnant. The atorvastatin component of CADUET may
cause fetal harm when administered to a pregnant woman. CADUET should be
administered to women of child-bearing potential only when such patients are
highly unlikely to conceive and have been informed of the potential hazards. If
the woman becomes pregnant while taking CADUET, it should be discontinued
immediately and the patient advised again as to the potential hazards to the
fetus, and the lack of known clinical benefit with continued use during
pregnancy.
Serum cholesterol and triglycerides increase during normal pregnancy, and
cholesterol products are essential for fetal development. Atherosclerosis is a
chronic process, and discontinuation of lipid-lowering drugs during pregnancy
should have little impact on long-term outcomes of primary hypercholesterolemia
therapy. Studies with amlodipine No evidence of teratogenicity or other embryo/fetal toxicity was
found when pregnant rats and rabbits were treated orally with amlodipine maleate
at doses up to 10 mg amlodipine/kg/day (respectively 8 times1 and 23 times1 the
maximum recommended human dose of 10 mg/day on a mg/m2
basis) during their respective periods of major organogenesis. However, litter
size was significantly decreased (by about 50%) and the number of intrauterine
deaths was significantly increased (about 5-fold) in rats receiving amlodipine
maleate at 10 mg amlodipine/kg/day for 14 days before mating and throughout
mating and gestation. Amlodipine maleate has been shown to prolong both the
gestation period and the duration of labor in rats at this dose. There are no
adequate and well-controlled studies in pregnant women. Studies with atorvastatin There are no adequate and well-controlled studies of atorvastatin
use during pregnancy. There have been rare reports of congenital anomalies
following intrauterine exposure to statins. In a review of about 100
prospectively followed pregnancies in women exposed to other statins, the
incidences of congenital anomalies, spontaneous abortions, and fetal
deaths/stillbirths did not exceed the rate expected in the general population.
However, this study was only able to exclude a three-to-four-fold increased risk
of congenital anomalies over background incidence. In 89% of these cases, drug
treatment started before pregnancy and stopped during the first trimester when
pregnancy was identified.
Atorvastatin crosses the rat placenta and reaches a level in fetal liver
equivalent to that of maternal plasma. Atorvastatin was not teratogenic in rats
at doses of atorvastatin calcium equivalent to up to 300 mg atorvastatin/kg/day
or in rabbits at doses of atorvastatin calcium equivalent to up to 100 mg
atorvastatin/kg/day. These doses resulted in multiples of about 30 times (rat)
or 20 times (rabbit) the human exposure based on surface area (mg/m2).
In a study in rats given atorvastatin calcium at doses equivalent to 20, 100,
or 225 mg atorvastatin/kg/day, from gestation day 7 through to lactation day 21
(weaning), there was decreased pup survival at birth, neonate, weaning, and
maturity for pups of mothers dosed with 225 mg/kg/day. Body weight was decreased
on days 4 and 21 for pups of mothers dosed at 100 mg/kg/day; pup body weight was
decreased at birth and at days 4, 21, and 91 at 225 mg/kg/day. Pup development
was delayed (rotorod performance at 100 mg/kg/day and acoustic startle at 225
mg/kg/day; pinnae detachment and eye opening at 225 mg/kg/day). These doses of
atorvastatin correspond to 6 times (100 mg/kg) and 22 times (225 mg/kg) the
human AUC at 80 mg/day. Labor and Delivery No studies have been conducted in pregnant women on the effect of
CADUET, amlodipine or atorvastatin on the mother or the fetus during labor or
delivery, or on the duration of labor or delivery. Amlodipine has been shown to
prolong the duration of labor in rats. Nursing MothersStudies with amlodipine It is not known whether the amlodipine component of CADUET is
excreted in human milk. Studies with atorvastatin It is not known whether the atorvastatin component of CADUET is
excreted in human milk, but a small amount of another drug in this class does
pass into breast milk. Nursing rat pups taking atorvastatin had plasma and liver
drug levels of 50% and 40%, respectively, of that in their mother's milk. Animal
breast milk drug levels may not accurately reflect human breast milk levels.
Because another drug in this class passes into human milk and because statins
have a potential to cause serious adverse reactions in nursing infants, women
taking CADUET, which includes atorvastatin, should be advised not to nurse their
infants (see CONTRAINDICATIONS). Pediatric Use There have been no studies conducted to determine the safety or
effectiveness of CADUET in pediatric populations. Studies with amlodipine The effect of amlodipine on blood pressure in patients less than
6 years of age is not known. Studies with atorvastatin Safety and effectiveness in patients 10–17 years of age with
heterozygous familial hypercholesterolemia have been evaluated in controlled
clinical trials of 6 months duration in adolescent boys and postmenarchal girls.
Patients treated with atorvastatin had an adverse experience profile generally
similar to that of patients treated with placebo, the most common adverse
experiences observed in both groups, regardless of causality assessment, were
infections. Doses greater than 20 mg have not been studied in
this patient population. In this limited controlled study, there was no
significant effect on growth or sexual maturation in boys or on menstrual cycle
length in girls. See CLINICAL PHARMACOLOGY, Clinical
Studies section; ADVERSE REACTIONS, Pediatric Patients;
and DOSAGE AND ADMINISTRATION,
Pediatric Patients (10–17 years of age) with Heterozygous Familial
Hypercholesterolemia. Adolescent females should be counseled on
appropriate contraceptive methods while on atorvastatin therapy (see CONTRAINDICATIONS and PRECAUTIONS, Pregnancy).
Atorvastatin has not been studied in controlled clinical trials
involving pre-pubertal patients or patients younger than 10 years of age.
Clinical efficacy with doses of atorvastatin up to 80 mg/day for 1 year have
been evaluated in an uncontrolled study of patients with homozygous FH including
8 pediatric patients. See CLINICAL PHARMACOLOGY,
Clinical Studies, Atorvastatin Effects in Homozygous Familial
Hypercholesterolemia. Geriatric Use There have been no studies conducted to determine the safety or
effectiveness of CADUET in geriatric populations. In studies with amlodipine Clinical studies of amlodipine did not include sufficient numbers
of subjects aged 65 and over to determine whether they respond differently from
younger subjects. Other reported clinical experience has not identified
differences in responses between the elderly and younger patients. In general,
dose selection of the amlodipine component of CADUET for an elderly patient
should be cautious, usually starting at the low end of the dosing range,
reflecting the greater frequency of decreased hepatic, renal, or cardiac
function, and of concomitant disease or other drug therapy. Elderly patients
have decreased clearance of amlodipine with a resulting increase of AUC of
approximately 40–60%, and a lower initial dose may be required (see DOSAGE AND
ADMINISTRATION). In studies with atorvastatin Of the 39,828 patients who received LIPITOR in clinical studies,
15,813 (40%) were ≥65 years old and 2,800 (7%) were ≥75 years old. No overall
differences in safety or effectiveness were observed between these subjects and
younger subjects, and other reported clinical experience has not identified
differences in responses between the elderly and younger patients, but greater
sensitivity of some older adults cannot be ruled out. Advanced age (≥65 years)
is a predisposing factor for myopathy.
Adverse Reactions
CADUET CADUET (amlodipine besylate/atorvastatin calcium) has been
evaluated for safety in 1092 patients in double-blind placebo controlled studies
treated for co-morbid hypertension and dyslipidemia. In general, treatment with
CADUET was well tolerated. For the most part, adverse experiences have been mild
or moderate in severity. In clinical trials with CADUET, no adverse experiences
peculiar to this combination have been observed. Adverse experiences are similar
in terms of nature, severity, and frequency to those reported previously with
amlodipine and atorvastatin.
The following information is based on the clinical experience with amlodipine
and atorvastatin. The Amlodipine Component of CADUET Amlodipine has been evaluated for safety in more than 11,000
patients in U.S. and foreign clinical trials. In general, treatment with
amlodipine was well tolerated at doses up to 10 mg daily. Most adverse reactions
reported during therapy with amlodipine were of mild or moderate severity. In
controlled clinical trials directly comparing amlodipine (N=1730) in doses up to
10 mg to placebo (N=1250), discontinuation of amlodipine due to adverse
reactions was required in only about 1.5% of patients and was not significantly
different from placebo (about 1%). The most common side effects are headache and
edema. The incidence (%) of side effects which occurred in a dose related manner
are as follows:
Adverse Event
amlodipine
2.5 mgN=275
5.0 mgN=296
10.0 mgN=268
PlaceboN=520
Edema
1.8
3.0
10.8
0.6
Dizziness
1.1
3.4
3.4
1.5
Flushing
0.7
1.4
2.6
0.0
Palpitations
0.7
1.4
4.5
0.6
Other adverse experiences which were not clearly dose related but which were
reported with an incidence greater than 1.0% in placebo-controlled clinical
trials include the following: Placebo-Controlled Studies
Adverse Event
amlodipine (%)(N=1730)
Placebo (%)(N=1250)
Headache
7.3
7.8
Fatigue
4.5
2.8
Nausea
2.9
1.9
Abdominal Pain
1.6
0.3
Somnolence
1.4
0.6
For several adverse experiences that appear to be drug and dose
related, there was a greater incidence in women than men associated with
amlodipine treatment as shown in the following table:
Adverse Event
amlodipine
Placebo
M=%(N=1218)
F=%(N=512)
M=%(N=914)
F=%(N=336)
Edema
5.6
14.6
1.4
5.1
Flushing
1.5
4.5
0.3
0.9
Palpitations
1.4
3.3
0.9
0.9
Somnolence
1.3
1.6
0.8
0.3
The following events occurred in ≤1% but >0.1% of patients treated with
amlodipine in controlled clinical trials or under conditions of open trials or
marketing experience where a causal relationship is uncertain; they are uled
to alert the physician to a possible relationship:
The following events occurred in ≤0.1% of patients treated with amlodipine in
controlled clinical trials or under conditions of open trials or marketing
experience: cardiac failure, pulse irregularity, extrasystoles, skin
discoloration, urticaria, skin dryness, alopecia, dermatitis, muscle weakness,
twitching, ataxia, hypertonia, migraine, cold and clammy skin, apathy,
agitation, amnesia, gastritis, increased appetite, loose stools, coughing,
rhinitis, dysuria, polyuria, parosmia, taste perversion, abnormal visual
accommodation, and xerophthalmia.
Other reactions occurred sporadically and cannot be distinguished from
medications or concurrent disease states such as myocardial infarction and
angina.
Amlodipine therapy has not been associated with clinically significant
changes in routine laboratory tests. No clinically relevant changes were noted
in serum potassium, serum glucose, total triglycerides, total cholesterol, HDL
cholesterol, uric acid, blood urea nitrogen, or creatinine.
In the CAMELOT and PREVENT studies (see CLINICAL PHARMACOLOGY Clinical Studies, Clinical Studies with
Amlodipine) the adverse event profile was
similar to that reported previously (see above), with the most common adverse
event being peripheral edema.
The following postmarketing event has been reported infrequently with
amlodipine treatment where a causal relationship is uncertain: gynecomastia. In
postmarketing experience, jaundice and hepatic enzyme elevations (mostly
consistent with cholestasis or hepatitis) in some cases severe enough to require
hospitalization have been reported in association with use of amlodipine.
Amlodipine has been used safely in patients with chronic obstructive
pulmonary disease, well-compensated congestive heart failure, peripheral
vascular disease, diabetes mellitus, and abnormal lipid profiles. 2These events occurred in less than 1% in placebo-controlled trials, but the
incidence of these side effects was between 1% and 2% in all multiple dose
studies. The Atorvastatin Component of CADUET The following serious adverse reactions are discussed in greater
detail in other sections of the label:Rhabdomyolysis and myopathy (see WARNINGS, Skeletal
Muscle)Liver enzyme abnormalities (see WARNINGS, Liver Dysfunction) Clinical Adverse Experiences Because clinical trials are conducted under widely varying
conditions, the adverse reaction rates observed in the clinical studies of a
drug cannot be directly compared to rates in the clinical trials of another drug
and may not reflect the rates observed in clinical practice.
In the LIPITOR placebo-controlled clinical trial database of 16,066 patients
(8755 LIPITOR vs. 7311 placebo; age range 10–93 years, 39% women, 91%
Caucasians, 3% Blacks, 2% Asians, 4% other) with a median treatment duration of
53 weeks, 9.7% of patients on LIPITOR and 9.5% of the patients on placebo
discontinued due to adverse reactions regardless of causality. The five most
common adverse reactions in patients treated with LIPITOR that led to treatment
discontinuation and occurred at a rate greater than placebo were: myalgia
(0.7%), diarrhea (0.5%), nausea (0.4%), alanine aminotransferase increase
(0.4%), and hepatic enzyme increase (0.4%).
The most commonly reported adverse reactions (incidence ≥ 2% and greater than
placebo) regardless of causality, in patients treated with LIPITOR in placebo
controlled trials (n=8755) were: nasopharyngitis (8.3%), arthralgia (6.9%),
diarrhea (6.8%), pain in extremity (6.0%), and urinary tract infection (5.7%).
Table 13 summarizes the frequency of clinical adverse reactions, regardless
of causality, reported in ≥ 2% and at a rate greater than placebo in patients
treated with LIPITOR (n=8755), from seventeen placebo-controlled trials.
Table 13. Clinical adverse reactions occurring in ≥ 2% in patents treated with any dose of LIPITOR and at an incidence greater than placebo regardless of causality (% of patients).
*Â Â Â Â Adverse Reaction greater than or equal to 2% in any dose greater than placebo
Other adverse reactions reported in placebo-controlled studies
include:
Body as a whole: malaise, pyrexia; Digestive system: abdominal discomfort, eructation,
flatulence, hepatitis, cholestasis; Musculoskeletal
system: musculoskeletal pain, muscle fatigue, neck pain, joint swelling;
Metabolic and nutritional system: transaminases
increase, liver function test abnormal, blood alkaline phosphatase increase,
creatine phosphokinase increase, hyperglycemia; Nervous
system: nightmare; Respiratory system:
epistaxis; Skin and appendages: urticaria; Special senses: vision blurred, tinnitus; Urogenital system: white blood cells urine positive. Anglo-Scandinavian Cardiac Outcomes Trial
(ASCOT) In ASCOT (see CLINICAL PHARMACOLOGY, Clinical
Studies, Clinical Studies with Atorvastatin) involving 10,305
participants (age range 40–80 years, 19% women; 94.6% Caucasians, 2.6% Africans,
1.5% South Asians, 1.3% mixed/other) treated with atorvastatin 10 mg daily
(n=5,168) or placebo (n=5,137), the safety and tolerability profile of the group
treated with atorvastatin was comparable to that of the group treated with
placebo during a median of 3.3 years of follow-up. Collaborative Atorvastatin Diabetes Study
(CARDS) In CARDS (see CLINICAL PHARMACOLOGY, Clinical
Studies, Clinical Studies with Atorvastatin) involving 2838 subjects
(age range 39–77 years, 32% women; 94.3% Caucasians, 2.4% South Asians, 2.3%
Afro-Caribbean, 1.0% other)with type 2 diabetes treated with LIPITOR 10 mg daily
(n=1428) or placebo (n=1410), there was no difference in the overall frequency
of adverse reactions or serious adverse reactions between the treatment groups
during a median follow-up of 3.9 years. No cases of rhabdomyolysis were
reported. Treating to New Targets Study (TNT) In TNT (see CLINICAL PHARMACOLOGY, Clinical
Studies) involving 10,001 subjects (age range 29–78 years, 19% women;
94.1% Caucasians, 2.9% Blacks, 1.0% Asians, 2.0% other) with clinically evident
CHD treated with LIPITOR 10 mg daily (n=5006) or LIPITOR 80 mg daily (n=4995),
there were more serious adverse reactions and discontinuations due to adverse
reactions in the high-dose atorvastatin group (92, 1.8%; 497, 9.9%,
respectively) as compared to the low-dose group (69, 1.4%; 404, 8.1%,
respectively) during a median follow-up of 4.9 years. Persistent transaminase
elevations (≥3 × ULN twice within 4–10 days) occurred in 62 (1.3%) individuals
with atorvastatin 80 mg and in nine (0.2%) individuals with atorvastatin 10 mg.
Elevations of CK (≥ 10 × ULN) were low overall, but were higher in the high-dose
atorvastatin treatment group (13, 0.3%) compared to the low-dose atorvastatin
group (6, 0.1%). Incremental Decrease in Endpoints Through Aggressive
Lipid Lowering Study (IDEAL) In IDEAL (see CLINICAL PHARMACOLOGY, Clinical
Studies) involving 8,888 subjects (age range 26–80 years, 19% women;
99.3% Caucasians, 0.4% Asians, 0.3% Blacks, 0.04% other) treated with LIPITOR 80
mg/day (n=4439) or simvastatin 20–40 mg daily (n=4449), there was no difference
in the overall frequency of adverse reactions or serious adverse reactions
between the treatment groups during a median follow-up of 4.8 years. Stroke Prevention by Aggressive Reduction in
Cholesterol Levels (SPARCL) In SPARCL involving 4731 subjects (age range 21–92 years, 40%
women; 93.3% Caucasians, 3.0% Blacks, 0.6% Asians, 3.1% other) without
clinically evident CHD but with a stroke or transient ischemic attack (TIA)
within the previous 6 months treated with LIPITOR 80 mg (n=2365) or placebo
(n=2366) for a median follow-up of 4.9 years, there was a higher incidence of
persistent hepatic transaminase elevations (≥ 3 × ULN twice within 4–10 days) in
the atorvastatin group (0.9%) compared to placebo (0.1%). Elevations of CK
(>10 Ă— ULN) were rare, but were higher in the atorvastatin group (0.1%)
compared to placebo (0.0%). Diabetes was reported as an adverse reaction in 144
subjects (6.1%) in the atorvastatin group and 89 subjects (3.8%) in the placebo
group (see PRECAUTIONS).
In a post-hoc analysis, LIPITOR 80 mg reduced the incidence of ischemic
stroke (218/2365, 9.2% vs. 274/2366, 11.6%) and increased the incidence of
hemorrhagic stroke (55/2365, 2.3% vs. 33/2366, 1.4%) compared to placebo. The
incidence of fatal hemorrhagic stroke was similar between groups (17 LIPITOR vs.
18 placebo). The incidence of non-fatal hemorrhagic strokes was significantly
greater in the atorvastatin group (38 non-fatal hemorrhagic strokes) as compared
to the placebo group (16 non-fatal hemorrhagic strokes). Subjects who entered
the study with a hemorrhagic stroke appeared to be at increased risk for
hemorrhagic stroke [7 (16%) LIPITOR vs. 2 (4%) placebo].
There were no significant differences between the treatment groups for
all-cause mortality: 216 (9.1%) in the LIPITOR 80 mg/day group vs. 211 (8.9%) in
the placebo group. The proportions of subjects who experienced cardiovascular
death were numerically smaller in the LIPITOR 80 mg group (3.3%) than in the
placebo group (4.1%). The proportions of subjects who experienced
non-cardiovascular death were numerically larger in the LIPITOR 80 mg group
(5.0%) than in the placebo group (4.0%). Postintroduction Reports with Atorvastatin The following adverse reactions have been identified during
postapproval use of the atorvastatin component of CADUET. Because these
reactions are reported voluntarily from a population of uncertain size, it is
not always possible to reliably estimate their frequency or establish a causal
relationship to drug exposure.
Adverse reactions associated with atorvastatin therapy reported since market
introduction, that are not uled above, regardless of causality assessment,
include the following: anaphylaxis, angioneurotic edema, bullous rashes
(including erythema multiforme, Stevens-Johnson syndrome, and toxic epidermal
necrolysis), rhabdomyolysis, fatigue, tendon rupture, hepatic failure,
dizziness, memory impairment, depression, and peripheral neuropathy. Pediatric Patients (ages 10–17 years) In a 26-week controlled study in boys and postmenarchal girls
(n=140, 31% female; 92% Caucasians, 1.6% Blacks, 1.6% Asians, 4.8% other), the
safety and tolerability profile of atorvastatin 10 to 20 mg daily was generally
similar to that of placebo (see CLINICAL PHARMACOLOGY, Clinical
Studies section and PRECAUTIONS, Pediatric Use).
Overdosage
There is no information on overdosage with CADUET in
humans. Information on Amlodipine Single oral doses of amlodipine maleate equivalent to 40 mg
amlodipine/kg and 100 mg amlodipine/kg in mice and rats, respectively, caused
deaths. Single oral amlodipine maleate doses equivalent to 4 or more mg
amlodipine/kg in dogs (11 or more times the maximum recommended clinical dose on
a mg/m2 basis) caused a marked peripheral vasodilation
and hypotension.
Overdosage might be expected to cause excessive peripheral vasodilation with
marked hypotension and possibly a reflex tachycardia. In humans, experience with
intentional overdosage of amlodipine is limited. Reports of intentional
overdosage include a patient who ingested 250 mg and was asymptomatic and was
not hospitalized; another (120 mg) was hospitalized, underwent gastric lavage
and remained normotensive; the third (105 mg) was hospitalized and had
hypotension (90/50 mmHg) which normalized following plasma expansion. A patient
who took 70 mg amlodipine and an unknown quantity of benzodiazepine in a suicide
attempt developed shock which was refractory to treatment and died the following
day with abnormally high benzodiazepine plasma concentration. A case of
accidental drug overdose has been documented in a 19-month-old male who ingested
30 mg amlodipine (about 2 mg/kg). During the emergency room presentation, vital
signs were stable with no evidence of hypotension, but a heart rate of 180 bpm.
Ipecac was administered 3.5 hours after ingestion and on subsequent observation
(overnight) no sequelae were noted.
If overdose should occur, begin active cardiac and respiratory monitoring.
Perform frequent blood pressure measurements. Should hypotension occur, initiate
cardiovascular support including elevation of the extremities and administration
of fluids. If hypotension remains unresponsive to these conservative measures,
consider administration of vasopressors (such as phenylephrine) with specific
attention to circulating volume and urine output. As amlodipine is highly
protein bound, hemodialysis is not likely to be of benefit. Information on Atorvastatin There is no specific treatment for atorvastatin overdosage. In
the event of an overdose, the patient should be treated symptomatically, and
supportive measures instituted as required. Due to extensive drug binding to
plasma proteins, hemodialysis is not expected to significantly enhance
atorvastatin clearance.
Dosage And Administration
Dosage of CADUET must be individualized on the basis of both
effectiveness and tolerance for each individual component in the treatment of
hypertension/angina and hyperlipidemia. Amlodipine (Hypertension or angina)Adults The usual initial antihypertensive oral dose of amlodipine is 5
mg once daily with a maximum dose of 10 mg once daily. Small, fragile, or
elderly individuals, or patients with hepatic insufficiency may be started on
2.5 mg once daily and this dose may be used when adding amlodipine to other
antihypertensive therapy.
Dosage should be adjusted according to each patient's need. In general,
titration should proceed over 7 to 14 days so that the physician can fully
assess the patient's response to each dose level. Titration may proceed more
rapidly, however, if clinically warranted, provided the patient is assessed
frequently.
The recommended dose of amlodipine for chronic stable or vasospastic angina
is 5–10 mg, with the lower dose suggested in the elderly and in patients with
hepatic insufficiency. Most patients will require 10 mg for adequate effect. See
ADVERSE REACTIONS
section for information related to dosage and side effects.
The recommended dose range of amlodipine for patients with coronary artery
disease is 5–10 mg once daily. In clinical studies the majority of patients
required 10 mg (see CLINICAL PHARMACOLOGY, Clinical
studies). Children The effective antihypertensive oral dose of amlodipine in
pediatric patients ages 6–17 years is 2.5 mg to 5 mg once daily. Doses in excess
of 5 mg daily have not been studied in pediatric patients (see CLINICAL
PHARMACOLOGY). Atorvastatin (Hyperlipidemia)Hyperlipidemia (Heterozygous Familial and
Nonfamilial) and Mixed Dyslipidemia (Fredrickson Types IIa and IIb) The recommended starting dose of atorvastatin is 10 or 20 mg once
daily. Patients who require a large reduction in LDL-C (more than 45%) may be
started at 40 mg once daily. The dosage range of atorvastatin is 10 to 80 mg
once daily. Atorvastatin can be administered as a single dose at any time of the
day, with or without food. The starting dose and maintenance doses of
atorvastatin should be individualized according to patient characteristics such
as goal of therapy and response (see current NCEP
Guidelines). After initiation and/or upon titration of atorvastatin,
lipid levels should be analyzed within 2 to 4 weeks and dosage adjusted
accordingly. Heterozygous Familial Hypercholesterolemia in
Pediatric Patients (10–17 years of age) The recommended starting dose of atorvastatin is 10 mg/day; the
maximum recommended dose is 20 mg/day (doses greater than 20 mg have not been
studied in this patient population). Doses should be individualized according to
the recommended goal of therapy (see current NCEP Pediatric Panel Guidelines3, CLINICAL PHARMACOLOGY,
and INDICATIONS AND
USAGE). Adjustments should be made at intervals of 4 weeks or
more. 3National Cholesterol Education Program (NCEP): Highlights of the Report of
the Expert Panel on Blood Cholesterol Levels in Children Adolescents. Pediatrics. 89(3):495–501. 1992. Homozygous Familial Hypercholesterolemia The dosage of atorvastatin in patients with homozygous FH is 10
to 80 mg daily. Atorvastatin should be used as an adjunct to other
lipid-lowering treatments (e.g., LDL apheresis) in these patients or if such
treatments are unavailable. Note: a 2.5/80 mg CADUET tablet is not available.
Management of patients needing a 2.5/80 mg combination requires individual
assessments of dyslipidemia and therapy with the individual components as a
2.5/80 mg CADUET tablet is not available. Concomitant Lipid Lowering Therapy Atorvastatin may be used with bile acid resins. Monitor for signs
of myopathy in patients receiving the combination of statins and fibrates (see
WARNINGS, Skeletal
Muscle, and PRECAUTIONS, Drug
Interactions). Dosage in Patients With Renal Impairment Renal disease does not affect the plasma concentrations nor LDL-C
reduction of atorvastatin; thus, dosage adjustment in patients with renal
dysfunction is not necessary (see WARNINGS, Skeletal Muscle, and CLINICAL PHARMACOLOGY, Specific
Populations). Dosage in Patients Taking Cyclosporine,
Clarithromycin, Itraconazole, or a Combination of Ritonavir plus Saquinavir or
Lopinavir plus Ritonavir In patients taking cyclosporine, therapy should be limited to
LIPITOR 10 mg once daily. In patients taking clarithromycin, itraconazole or in
patients with HIV taking a combination of ritonavir plus saquinavir or lopinavir
plus ritonavir, for doses of atorvastatin exceeding 20 mg, appropriate clinical
assessment is recommended to ensure that the lowest dose necessary of
atorvastatin is employed (see WARNINGS, Skeletal Muscle, and PRECAUTIONS, Drug
Interactions). CADUET CADUET may be substituted for its individually titrated
components. Patients may be given the equivalent dose of CADUET or a dose of
CADUET with increased amounts of amlodipine, atorvastatin or both for additional
antianginal effects, blood pressure lowering, or lipid lowering effect.
CADUET may be used to provide additional therapy for patients already on one
of its components. As initial therapy for one indication and continuation of
treatment of the other, the recommended starting dose of CADUET should be
selected based on the continuation of the component being used and the
recommended starting dose for the added monotherapy.
CADUET may be used to initiate treatment in patients with hyperlipidemia and
either hypertension or angina. The recommended starting dose of CADUET should be
based on the appropriate combination of recommendations for the monotherapies.
The maximum dose of the amlodipine component of CADUET is 10 mg once daily. The
maximum dose of the atorvastatin component of CADUET is 80 mg once daily.
See above for detailed information related to the dosing and administration
of amlodipine and atorvastatin.
How Supplied
CADUET tablets contain amlodipine besylate and atorvastatin
calcium equivalent to amlodipine and atorvastatin in the dose strengths
described below.
CADUET tablets are differentiated by tablet color/size and are engraved with
"Pfizer" on one side and a unique number on the other side. CADUET tablets are
supplied for oral administration in the following strengths and package
configurations:
Read the patient information that comes with CADUET before you start taking
it, and each time you get a refill. There may be new information. This
information does not replace talking with your doctor about your condition or
treatment. If you have any questions about CADUET, ask your doctor or
pharmacist.
What is CADUET?
CADUET is a prescription drug that combines Norvasc®
(amlodipine besylate) and Lipitor® (atorvastatin calcium)
in one pill.
CADUET is used in adults who need both Norvasc and
Lipitor.
Norvasc is used to treat:
High blood pressure (hypertension) and
Chest pain (angina) and
Blocked arteries of the heart (coronary artery disease)
Lipitor is used to lower the levels of "bad" cholesterol and triglycerides in
your blood. It can also raise the levels of "good" cholesterol.
Lipitor is also used to lower the risk for heart attack, stroke, certain
types of heart surgery, and chest pain in patients who have heart disease or
risk factors for heart disease such as:
age, smoking, high blood pressure, low HDL-C, heart disease in the family
Lipitor can lower the risk for heart attack or stroke in patients with
diabetes and risk factors such as:
diabetic eye or kidney problems, smoking, or high blood pressure.
CADUET has not been studied in children.
Who should not use CADUET?
Do not use CADUET if
you:
Are pregnant or think you may be pregnant, or are planning to become
pregnant. CADUET may harm your unborn baby. If you get pregnant, stop taking
CADUET and call your doctor right away.
Are breastfeeding. CADUET can pass into your breast milk and may harm your
baby. Do not breastfeed if you take CADUET.
Have liver problems.
Are allergic to anything in CADUET. The active ingredients are atorvastatin
calcium and amlodipine besylate. See the end of this leaflet for a complete ul
of ingredients.
What should I tell my doctor before taking CADUET?
Tell your doctor about all of your health conditions,
including, if you have:
heart disease
muscle aches or weakness
diabetes
thyroid problems
kidney problems
or drink more than 2 glasses of alcohol daily
Tell your doctor about all the medicines you take including prescription and
nonprescription medicines, vitamins and herbal supplements. CADUET and some
other medicines can interact, causing serious side effects. Especially tell your
doctor if you take medicines for:
your immune system
infections
cholesterol
birth control
heart failure
HIV (AIDS)
You can use nitroglycerin and CADUET together. If you take nitroglycerin for
chest pain (angina), do not stop taking it while taking CADUET.
Know all the medicines you take. Keep a ul of them with you to show your
doctor and pharmacist.
How should I take CADUET?
Take CADUET once a day, exactly as your doctor tells you. Do not change your
dose or stop CADUET without talking to your doctor.
Take CADUET each day at any time of day, at about the same time each day.
CADUET can be taken with or without food.
Do not break the tablets before taking them. Talk to your doctor if you have
a problem swallowing pills.
Your doctor should start you on a low-fat diet before giving you CADUET.
Stay on this low-fat diet when you take CADUET.
CADUET comes in many different strengths. Your doctor will test your
cholesterol and blood pressure to find the right dose for you.
If you miss a dose, take it as soon as you remember. Do not take CADUET if
it has been more than 12 hours since your missed dose. Just take the next dose
at your regular time. Do not take 2 doses of CADUET at the same time.
If too much CADUET is taken by accident, call your doctor or poison control
center, or go to the nearest emergency room.
What should I avoid while taking CADUET?
Avoid getting pregnant. If you get pregnant, stop taking CADUET right away
and call your doctor.
Do not breastfeed. CADUET can pass into your breast milk and may harm your
baby.
What are possible side effects of CADUET?
CADUET can cause serious side effects. These side effects
happen only to a small number of people. Your doctor can monitor you for them.
These side effects usually go away if your dose is lowered or CADUET is stopped.
These serious side effects include:
Muscle problems. CADUET can cause serious muscle
problems that can lead to kidney problems, including kidney failure. You have a
higher chance for muscle problems if you are taking certain other medicines with
CADUET.
Liver problems. CADUET can cause liver problems.
Your doctor may do blood tests to check your liver before you start taking
CADUET and while you take it.
Call your doctor right away if:
you have muscle problems like weakness, tenderness, or pain that happen
without a good reason, especially if you also have a fever or feel more tired
than usual
allergic reactions including swelling of the face, lips, tongue, and/or
throat that may cause difficulty in breathing or swallowing which may require
treatment right away.
you have nausea and vomiting, stomach pain
you are passing brown or dark-colored urine
you feel more tired than usual
your skin and white of your eyes get yellow
allergic skin reactions.
Chest pain that does not go away or gets worse.
Sometimes, when you start CADUET or increase your dose, chest pain can get worse
or a heart attack can happen. If this happens, call your doctor or go to the
emergency room right away.
Common side effects of CADUET include:
headache
tiredness
stomach pain
upset stomach
swelling of your legs or ankles (edema)
hot or warm feeling in your face (flushing)
irregular heartbeat (arrhythmia)
very fast heartbeat (heart palpitations)
muscle and joint pain
alterations in some laboratory blood tests
dizziness
extreme sleepiness
nausea
diarrhea
Additional side effects have been reported: tendon problems.
Talk to your doctor or pharmacist about side effects that bother you or do
not go away.
There are other side effects of CADUET. Ask your doctor or pharmacist for a
complete ul.
How do I store CADUET?
Store CADUET at room temperature, 68 to 77°F (20 to
25°C).
Do not keep medicine that is out-of-date or that you no
longer need.
Keep CADUET and all medicines out of the reach of children. Keep medicines in places where children cannot get it.
General information about CADUET
Medicines are sometimes prescribed for conditions that are
not mentioned in patient information leaflets. Do not use CADUET for a condition
for which it was not prescribed. Do not give CADUET to other people, even if
they have the same problem you have. It may harm them.
This leaflet summarizes the most important information about
CADUET. If you want more information, talk with your doctor. Ask your doctor or
pharmacist for information about CADUET written for health professionals. You
can also go to the CADUET website at www.CADUET.com, or call 866-514-0900.
What is high blood pressure (hypertension)?
You have high blood pressure when the force of blood against the walls of
your arteries stays high. This can damage your heart and other parts of your
body. Drugs that lower blood pressure lower your risk of having a stroke or
heart attack.
What is angina (chest pain)?
Angina is a pain that keeps coming back when part of your heart does not get
enough blood. It feels like something is pressing or squeezing your chest under
the breastbone. Sometimes you can feel it in your shoulders, arms, neck, jaw, or
back.
What is cholesterol?
Cholesterol is a fat-like substance made in your body. It is also found in
foods. You need some cholesterol for good health, but too much is not good for
you. Cholesterol can clog your blood vessels.
What is a heart attack?
A heart attack occurs when heart muscle does not get enough blood. Symptoms
include chest pain, trouble breathing, nausea, and weakness. Heart muscle cells
may be damaged or die. The heart cannot pump well or may stop beating.
What is a stroke?
A stroke occurs when nerve cells in the brain do not get enough blood. The
cells may be damaged or die. The damaged cells may cause weakness or problems
speaking or thinking.
WHAT ARE THE INGREDIENTS IN CADUET?
Active ingredients: amlodipine besylate, atorvastatin
calcium
Film coating: Opadry® II White 85F28751 (polyvinyl
alcohol, titanium dioxide, PEG 3000 and talc) or Opadry® II Blue 85F10919
(polyvinyl alcohol, titanium dioxide, PEG 3000, talc, and FD&C blue #2)
Rx only
Manufactured by Pfizer Ireland PharmaceuticalsDublin, Ireland LAB-0347-3.0July 2009
"This tool does not provide medical advice, and is for informational and educational purposes only, and is not a substitute for professional medical advice, treatment or diagnosis. Call your doctor to receive medical advice. If you think you may have a medical emergency, please dial 911."
"Do not rely on openFDA to make decisions regarding medical care. While we make every effort to ensure that data is accurate, you should assume all results are unvalidated. We may limit or otherwise restrict your access to the API in line with our Terms of Service."
"This product uses publicly available data from the U.S. National Library of Medicine (NLM), National Institutes of Health, Department of Health and Human Services; NLM is not responsible for the product and does not endorse or recommend this or any other product."
PillSync may earn a commission via links on our site

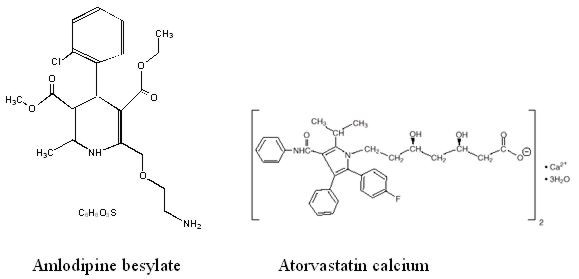
Figure 2 – Effects on primary endpoint of amlodipine versus placebo across sub-groups
Table 4 below summarizes the significant composite endpoint and clinical outcomes from the composites of the primary endpoint. The other components of the primary endpoint including cardiovascular death, resuscitated cardiac arrest, myocardial infarction, hospitalization for heart failure, stroke/TIA, or peripheral vascular disease did not demonstrate a significant difference between amlodipine and placebo.