Cesamet (nabilone 1 mg) Dailymed

IMPRINT: MEDA 1221 SHAPE: capsule

Go PRO for all pill images
Description
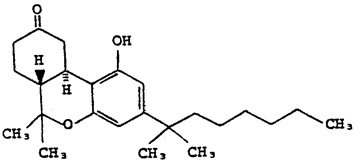
Cesamet® (nabilone) is a synthetic cannabinoid for oral administration. Nabilone as a raw material occurs as a white to off-white polymorphic crystalline powder. In aqueous media, the solubility of nabilone is less than 0.5 mg/L, with pH values ranging from 1.2 to 7.0.
Chemically, nabilone is similar to the active ingredient found in naturally occurring Cannabis sativa L. [Marijuana; delta-9-tetrahydrocannabinol (delta-9-THC)]. Nabilone is (±)-trans-3-(1,1-dimethylheptyl)-6,6a,7,8,10,10a-hexahydro-1-hydroxy-6-6-dimethyl-9H-dibenzo[b,d]pyran-9-one and has the empirical formula C24H36O3. It has a molecular weight of 372.55. The structural formula is as follows:
Each 1 mg Cesamet capsule contains 1 mg of nabilone and the following inactive ingredients: povidone and corn starch. The capsule shells contain the following inactive ingredients: FD&C Blue No. 2 (indigo carmine), red iron oxide, gelatin, and titanium dioxide.
Clinical Pharmacology
Pharmacodynamics
Cesamet (nabilone) is an orally active synthetic cannabinoid which, like other cannabinoids, has complex effects on the central nervous system (CNS). It has been suggested that the antiemetic effect of nabilone is caused by interaction with the cannabinoid receptor system, i.e., the CB (1) receptor, which has been discovered in neural tissues.
Nontherapeutic Effects: Cesamet, a synthetic cannabinoid, has the potential to be abused and to produce psychological dependence. Cesamet has complex effects on the central nervous system. Its effects on the mental state (i.e., “inner mental life”) are similar to those of cannabis. Subjects given Cesamet may experience changes in mood (euphoria, detachment, depression, anxiety, panic, paranoia), decrements in cognitive performance and memory, a decreased ability to control drives and impulses, and alterations in the experience of reality (e.g., distortions in the perception of objects and the sense of time, hallucinations). These phenomena appear to be more common when larger doses of Cesamet are administered; however, a full-blown picture of psychosis (psychotic organic brain syndrome) may occur in patients receiving doses within the lower portion of the therapeutic range.
Data on the chronic use of Cesamet are not available; experience with cannabis suggests that chronic use of cannabinoids may be associated with a variety of untoward effects on motivation, cognition, judgment, as well as other mental status changes. Whether these phenomena reflect the underlying character of individuals chronically abusing cannabis or are a result of the use of cannabis is not known.
The simultaneous use of Cesamet and alcohol or barbiturates may produce additive depressive effects on central nervous system function. Possible changes in mood and other adverse behavioral effects may occur in patients receiving Cesamet. Patients should remain under supervision of a responsible adult while using Cesamet.
Cesamet has central nervous system activity. It produces relaxation, drowsiness, and euphoria in the recommended dosage range. Tolerance to these effects develops rapidly and is readily reversible.
In addition to effects on the mental state, Cesamet has several systemic actions; most prominent are dry mouth and hypotension. Cesamet has been observed to elevate supine and standing heart rates and to cause supine and orthostatic hypotension. In clinical studies, oral administration of 2 mg of Cesamet did produce some decrease in airway resistance in normal controls but had no effect in patients with asthma. No other nontherapeutic effects of clinical significance due to Cesamet have been reported.
Pharmacokinetics
Absorption and Distribution: Cesamet (nabilone) appears to be completely absorbed from the human gastrointestinal tract when administered orally. Following oral administration of a 2 mg dose of radiolabeled nabilone, peak plasma concentrations of approximately 2 ng/mL nabilone and 10 ng equivalents/mL total radioactivity are achieved within 2.0 hours. The plasma half-life (T½) values for nabilone and total radioactivity of identified and unidentified metabolites are about 2 and 35 hours, respectively. The initial rapid disappearance of radioactivity represents uptake and distribution of nabilone into tissue and the slower phase elimination by metabolism and excretion. The apparent volume of distribution of nabilone is about 12.5 L/kg.
Nabilone exhibits dose linearity within its therapeutic range. Clinical data suggests that the intake of food does not significantly affect either the rate or extent of absorption.
Metabolism: Metabolism of nabilone is extensive and several metabolites have been identified. Precise information concerning the metabolites that may accumulate is not available. The relative activities of the metabolites and the parent drug have not been established. There are at least two metabolic pathways involved in the biotransformation of nabilone. A minor pathway is initiated by the stereospecific enzymatic reduction of the 9-keto moiety of nabilone to produce the isomeric carbinol metabolite. The peak concentrations of nabilone and its carbinol metabolites are comparable, but their combined exposures in plasma do not account for more than 20% of that of total radioactivity. Secondly, a metabolite of nabilone in feces has been identified as a diol formed by reduction of the 9-keto group plus oxidation at the penultimate carbon of the dimethylheptyl side chain. In addition, there is evidence of extensive metabolism of Cesamet by multiple P450 enzyme isoforms. In vitro P450 inhibition studies using human liver microsomes showed that nabilone did not significantly inhibit CYP1A2, 2A6, 2C19, 2D6, and 3A4 (using midazolam and nifedipine as substrates). Nabilone had a weak inhibitory effect on CYP 2E1 and 3A4 (testosterone; IC50> 50 µM) and had a moderate inhibitory effect on CYP2C8 and 2C9 (IC50> 10 µM). However, in clinical use, the very low nabilone plasma concentration is unlikely to interfere with the P450-mediated degradation of co-administered drugs. Chronic oral administration of 1 mg t.i.d. for 14 days to 3 subjects gave no indication there was any significant accumulation of nabilone. Available evidence suggests that one or more of the metabolites has a terminal elimination half-life that exceeds that of nabilone. Consequently, in repeated use, the metabolites may accumulate at concentrations in excess of the parent drug.
Elimination: The route and rate of the elimination of nabilone and its metabolites are similar to those observed with other cannabinoids, including delta-9-THC (dronabinol). When nabilone is administered intravenously, the drug and its metabolites are eliminated mainly in the feces (approximately 67%) and to a lesser extent in the urine (approximately 22%) within 7 days. Of the 67% recovered from the feces, 5% corresponded to the parent compound and 16% to its carbinol metabolite. Following oral administration about 60% of nabilone and its metabolites were recovered in the feces and about 24% in urine. Therefore, it appears that the major excretory pathway is the biliary system.
The effects of age, gender, hepatic dysfunction, and renal insufficiency on the metabolism and elimination of nabilone have not been determined.
Special Populations: The pharmacokinetic profile of Cesamet has not been investigated in either pediatric (see PRECAUTIONS, Pediatric Use ) or geriatric patients (see PRECAUTIONS, Geriatric Use ).
Clinical Trials
Cesamet was evaluated for its effectiveness and safety in the treatment of nausea and vomiting induced by cancer chemotherapy in patients receiving a wide variety of chemotherapy regimens, including low-dose cisplatin (20 mg/m2) in both placebo-controlled and active controlled (prochlorperazine) trials.
During Cesamet treatment patients reported a higher incidence of adverse effects. The most frequent were drowsiness, vertigo, dry mouth and euphoria. However, most of the adverse effects occurring with Cesamet were of mild to moderate severity (see ADVERSE REACTIONS ).
Indications And Usage
Cesamet capsules are indicated for the treatment of the nausea and vomiting associated with cancer chemotherapy in patients who have failed to respond adequately to conventional antiemetic treatments. This restriction is required because a substantial proportion of any group of patients treated with Cesamet can be expected to experience disturbing psychotomimetic reactions not observed with other antiemetic agents.
Because of its potential to alter the mental state, Cesamet is intended for use under circumstances that permit close supervision of the patient by a responsible individual particularly during initial use of Cesamet and during dose adjustments.
Cesamet contains nabilone, which is controlled in Schedule II of the Controlled Substances Act. Schedule II substances have a high potential for abuse. Prescriptions for Cesamet should be limited to the amount necessary for a single cycle of chemotherapy (i.e., a few days).
Cesamet capsules are not intended to be used on as needed basis or as a first antiemetic product prescribed for a patient.
As with all controlled drugs, prescribers should monitor patients receiving nabilone for signs of excessive use, abuse and misuse. Patients who may be at increased risk for substance abuse include those with a personal or family history of substance abuse (including drug or alcohol abuse) or mental illness.
Contraindications
Cesamet is contraindicated in any patient who has a history of hypersensitivity to any cannabinoid.
Warnings
• The effects of Cesamet may persist for a variable and unpredictable period of time following its oral administration. Adverse psychiatric reactions can persist for 48 to 72 hours following cessation of treatment.• Cesamet has the potential to affect the CNS, which might manifest itself in dizziness, drowsiness, euphoria “high”, ataxia, anxiety, disorientation, depression, hallucinations and psychosis.• Cesamet can cause tachycardia and orthostatic hypotension.• Because of individual variation in response and tolerance to the effects of Cesamet, patients should remain under supervision of a responsible adult especially during initial use of Cesamet and during dose adjustments.• Patients receiving treatment with Cesamet should be specifically warned not to drive, operate machinery, or engage in any hazardous activity while receiving Cesamet.• Cesamet should not be taken with alcohol, sedatives, hypnotics, or other psychoactive substances because these substances can potentiate the central nervous system effects of nabilone.
Precautions
General
The benefit/risk ratio of Cesamet use should be carefully evaluated in patients with the following medical conditions because of individual variation in response and tolerance to the effects of Cesamet.
• Since Cesamet can elevate supine and standing heart rates and cause postural hypotension, it should be used with caution in the elderly, and in patients with hypertension or heart disease.• Cesamet should also be used with caution in patients with current or previous psychiatric disorders, (including manic depressive illness, depression, and schizophrenia) as the symptoms of these disease states may be unmasked by the use of cannabinoids.• Cesamet should be used with caution in individuals receiving concomitant therapy with sedatives, hypnotics, or other psychoactive drugs because of the potential for additive or synergistic CNS effects.• Cesamet should be used with caution in patients with a history of substance abuse, including alcohol abuse or dependence and marijuana use, since Cesamet contains a similar active compound to marijuana.• The safety aspects of the effects of hepatic and renal impairment have not been investigated.• Nabilone is purportedly highly bound to plasma proteins and undergoes extensive first pass hepatic metabolism. Those properties have the potential to lead to drug-drug interactions affecting the pharmacokinetics of similar behaving co-administered drugs or of Cesamet itself.• The effects of QT prolongation potential by Cesamet have not been determined.• Cesamet should be used with caution in pregnant patients, nursing mothers, or pediatric patients because it has not been studied in these patient populations.Information for Patients
Persons taking Cesamet should be alerted to the potential for additive central nervous system depression resulting from simultaneous use of Cesamet and alcohol or other central nervous system depressants such as benzodiazepines and barbiturates. This combination should be avoided. Patients receiving treatment with Cesamet should be specifically warned not to drive, operate machinery, or engage in any hazardous activity. Patients using Cesamet should be made aware of possible changes in mood and other adverse behavioral effects of the drug so as to avoid panic in the event of such manifestations. Patients should remain under supervision of a responsible adult while using Cesamet.
Drug Interactions
Potential interactions between Cesamet 2 mg, and diazepam 5 mg; sodium secobarbital 100 mg; alcohol 45 mL (absolute laboratory alcohol); or codeine 65 mg, were evaluated in 15 subjects. Only a single combination was utilized at any one time. The subjects were evaluated according to physiologic (i.e., heart rate and blood pressure), psychometric, psychomotor, and subjective parameters. In this study, as expected, the depressant effects of the combinations were additive. Psychomotor function was particularly impaired with concurrent use of diazepam. Caution must thus be used when administering nabilone in combination with any CNS depressant.
Nabilone is purportedly highly bound to plasma proteins, and therefore, might displace other protein-bound drugs. Therefore, practitioners should monitor patients for a change in dosage requirements when administering nabilone to patients receiving other highly protein-bound drugs. Published reports of drug-drug interactions involving cannabinoids are summarized in the following table.
CONCOMITANT DRUG
CLINICAL EFFECT(S)
Amphetamines, cocaine, other sympathomimeticagents
Additive hypertension, tachycardia, possibly cardiotoxicity
Atropine, scopolamine, antihistamines, otheranticholinergic agents
Additive or super-additive tachycardia, drowsiness
Amitriptyline, amoxapine, desipramine, othertricyclic antidepressants
Additive tachycardia, hypertension, drowsiness
Barbiturates, benzodiazepines, ethanol, lithium,opioids, buspirone, antihistamines, muscle relaxants,other CNS depressants
Additive drowsiness and CNS depression
Disulfiram
A reversible hypomanic reaction was reported in a 28 y/oman who smoked marijuana; confirmed by dechallenge andrechallenge
Fluoxetine
A 21 y/o female with depression and bulimia receiving 20mg/day fluoxetine X 4 wks became hypomanic aftersmoking marijuana; symptoms resolved after 4 days
Antipyrine, barbiturates
Decreased clearance of these agents, presumably viacompetitive inhibition of metabolism
Theophylline
Increased theophylline metabolism reported with smoking ofmarijuana; effect similar to that following smoking tobacco
Opioids
Cross-tolerance and mutual potentiation
Naltrexone
Oral THC effects were enhanced by opioid receptorblockade.
Alcohol
Increase in the positive subjective mood effects of smokedmarijuana
Animal Pharmacology and/or Toxicology
Monkeys treated with Cesamet at doses as high as 2 mg/kg/day for a year experienced no significant adverse events. This result contrasts with the findings in a planned 1-year dog study that was prematurely terminated because of deaths associated with convulsions in dogs receiving as little as 0.5 mg/kg/day. The earliest deaths, however, occurred at 56 days in dogs receiving 2 mg/kg/day. The unusual vulnerability of the dog to Cesamet is not understood; it is hypothesized, however, that the explanation lies in the fact that the dog differs markedly from other species in its metabolism of Cesamet.
Carcinogenesis, Mutagenesis, Impairment of Fertility
No long-term studies in animals have been performed to evaluate the carcinogenic potential of nabilone.
Nabilone was not genotoxic in the Ames test, the rat hepatocyte unscheduled DNA synthesis (UDS) test, the Chinese hamster bone marrow cell sister chromatid exchange (SCE) test, the male rat dominant lethal tests nor the rat micronucleus test.
Dietary administration of nabilone up to 4 mg/kg/day (about 6 times the recommended maximum human dose based on body surface area) was found to have no effect on fertility and reproductive performance of male and female rats.
Pregnancy: Teratogenic Effects
Teratology studies conducted in pregnant rats at doses up to 12 mg/kg/day (about 16 times the human dose on a body surface area basis) and in pregnant rabbits at doses up to 3.3 mg/kg/day (about 9 times the human dose on a body surface area basis) did not disclose any evidence for a teratogenic potential of nabilone. However, there was dose related developmental toxicity in both species as evidenced by increases in embryo lethality, fetal resorptions, decreased fetal weights and pregnancy disruptions. In rats, postnatal developmental toxicity was also observed. There are no adequate and well-controlled studies in pregnant women. Because animal studies cannot rule out the possibility of harm, Cesamet should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.
Nursing Mothers
It is not known whether this drug is excreted in breast milk. Because many drugs including some cannabinoids are excreted in breast milk it is not recommended that Cesamet be given to nursing mothers.
Pediatric Use
Safety and effectiveness have not been established in patients younger than 18 years of age. Caution is recommended in prescribing Cesamet to children because of psychoactive effects.
Geriatric Use
Clinical studies of Cesamet did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from younger subjects. In general, dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy. Cesamet should be used with caution in elderly patients aged 65 and over because they are generally more sensitive to the psychoactive effects of drugs and Cesamet can elevate supine and standing heart rates and cause postural hypotension.
Adverse Reactions
Commonly Encountered Reactions: During controlled clinical trials of Cesamet, virtually all patients experienced at least one adverse reaction. The most commonly encountered events were drowsiness, vertigo, dry mouth, euphoria (feeling “high”), ataxia, headache, and concentration difficulties.
Comparative Incidence of Reactions: Accurate estimates of the incidence of adverse events associated with the use of any drug are difficult to obtain. Estimates are influenced by factors such as drug dose, detection technique, setting, and physician judgments, among others. Consequently, the tables presented below are presented solely to indicate the relative frequency of adverse events reported in representative controlled clinical studies conducted to evaluate the safety and efficacy of Cesamet under relatively similar conditions of use. The figures cited cannot be used to predict precisely the incidence of untoward events in the course of usual medical practice, in which patient characteristics and other factors may differ from those that prevailed in the clinical trials. These incidence figures also cannot be compared with those obtained from other clinical studies involving related drug products because each group of drug trials is conducted under a different set of conditions.
Finally, it is important to emphasize that these tabulations do not reflect the relative severity and/or clinical importance of the adverse events. A better perspective on the serious adverse events associated with the use of Cesamet is provided in the WARNINGS and PRECAUTIONS sections.
The following tables ul in order of decreasing frequency the adverse reactions encountered by a substantial proportion of patients treated with Cesamet participating in representative controlled clinical trials.
Incidence of Adverse Reactions in Placebo-Controlled Studies
Â
Nabilone (n=132)
Placebo (n=119)
Adverse Event
Patients
Percent
Patients
Percent
Vertigo
69
52
3
3
Drowsiness
69
52
6
5
Dry Mouth
47
36
2
2
Ataxia
19
14
0
0
Euphoria
14
11
1
1
Sleep Disturbance
14
11
1
1
Dysphoria
12
9
0
0
Headache
8
6
0
0
Nausea
5
4
0
0
Disorientation
3
2
0
0
Depersonalization
2
2
1
1
Incidence of Adverse Reactions in Active-Controlled Studies
Â
Nabilone (n=250)
Prochlorperazine (n=232)
Adverse Event
Patients
Percent
Patients
Percent
Drowsiness
165
66
108
47
Vertigo/Dizziness
147
59
53
23
Euphoria
95
38
12
5
Dry Mouth
54
22
11
5
Depression
35
14
37
16
Ataxia
32
13
4
2
Visual Disturbance
32
13
9
4
Concentration Difficulties
31
12
3
1
Hypotension
20
8
3
1
Asthenia
19
8
10
4
Anorexia
19
8
22
9
Headache
18
7
14
6
Sedation
7
3
2
1
Increased Appetite
6
2
2
1
Adverse Reactions by Body System—The following ul of adverse events is organized by decreasing frequency within body systems for patients treated with Cesamet in controlled clinical trials. All events are uled regardless of causality assessment.
Blood and Hematopoietic—Anemia
Cardiovascular—Orthostatic hypotension, hypotension, tachycardia, syncope, palpitation, flushing, hypertension, arrhythmia, and cerebral vascular accident.
Eye and Ear—Vision disturbance, ear tightness, eye irritation, eye dryness, equilibrium dysfunction, tinnitus, eye disorder, amblyopia, eye swelling, eyelid diseases, pupil dilation, photophobia, and visual field defect.
Gastrointestinal—Dry mouth, nausea, anorexia, vomiting, diarrhea, abdominal pain, constipation, aphthous ulcer, mouth irritation, gastritis, and dyspepsia.
Genitourinary—Increased urination, decreased urination, hot flashes, urinary retention, and frequency of micturition.
Infection—Bacterial infection
Metabolic and Endocrine—Thirst
Musculoskeletal—Muscle pain, back pain, neck pain, joint pain, and unspecified pain.
Nervous System—Drowsiness, vertigo, ataxia, decreased concentration, sedation, hallucinations, paresthesia, tremor, memory disturbance, perception disturbance, convulsions, dystonia, numbness, and akathisia.
Psychiatric—Euphoria (feeling “high”), sleep disturbance, depression, confusion, disorientation, anxiety, depersonalization syndrome, speech disorder, abnormal dreams, insomnia, mood swings, inebriated feeling, toxic psychosis, paranoia, apathy, thought disorder, withdrawal, panic disorder, phobic neurosis, emotional disorder, and hyperactivity.
Respiratory—Dyspnea, pharyngitis, nasal congestion, sinus headache, thick tongue, dry throat, dry nose, wheezing, nosebleed, cough, voice change, and chest pain.
Skin and Appendages—Anhidrosis, photosensitivity, pruritus, rash, and allergic reactions.
Miscellaneous and Ill-Defined Conditions—Headache, fatigue, lightheadedness, coordination disturbance, asthesia, dysphoria, dizziness, taste change, excessive appetite, chills, excessive sweating, nervousness, malaise, postural dizziness, twitch, irritability, fever, inhibited walking, unconsciousness, hypotonia, and impaired urination.
Postmarketing Adverse Reactions—Cesamet has been marketed internationally since 1982. The following adverse reactions uled in order of decreasing frequency by body system have been reported since Cesamet has been marketed. All events are uled regardless of causality assessment.
Blood and Hematopoietic—Leukopenia
Cardiovascular—Hypotension and tachycardia
Eye and Ear—Visual disturbances
Gastrointestinal—Dry mouth, nausea, vomiting, and constipation
Nervous System—Hallucinations, CNS depression, CNS stimulation, ataxia, stupor, vertigo, convulsion, and circumoral paresthesia
Psychiatric—Somnolence, confusion, euphoria, depression, dysphoria, depersonalization, anxiety, psychosis, and emotional lability
Miscellaneous and Ill-Defined Conditions—Dizziness, headache, insomnia, abnormal thinking, chest pain, lack of effect, and face edema
To report SUSPECTED ADVERSE REACTIONS, contact Bausch Health US, LLC at 1-800-321-4576 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Drug Abuse And Dependence
Controlled Substance—Cesamet, a synthetic cannabinoid pharmacologically related to Cannabis sativa L. (Marijuana; (delta-9-THC) is a highly abusable substance. Cesamet is controlled under Schedule II (CII) of the Controlled Substances Act. Prescriptions for Cesamet should be limited to the amount necessary for a single cycle of chemotherapy (i.e., a few days). Cesamet may produce subjective side effects which may be interpreted as a euphoria or marijuana-like “high” at therapeutic doses.
It is not known what proportion of individuals exposed chronically to Cesamet or other cannabinoids will develop either psychological or physical dependence. Long term use of these compounds has, however, been associated with disorders of motivation, judgment, and cognition. It is not clear, though, if this is a manifestation of the underlying personalities of chronic users of this class of drugs or if cannabinoids are directly responsible for these effects. An abstinence syndrome has been reported following discontinuation of delta-9-THC at high doses of 200 mg per day for 12 to 16 consecutive days. The acute phase was characterized by psychic distress, insomnia, and signs of autonomic hyperactivity (sweating, rhinorrhea, loose stools, hiccups). A protracted abstinence phase may have occurred in subjects who reported sleep disturbances for several weeks after delta-9-THC discontinuation.
Abuse—Cesamet may produce subjective side effects that may be interpreted as a euphoria or marijuana-like “high” at therapeutic doses. Cesamet was shown to be qualitatively and quantitatively similar to delta-9-THC in the production of cannabis-like effects, thus demonstrating that Cesamet has a high potential for abuse.
Preclinical studies performed in both dogs and monkeys demonstrated that Cesamet was cannabinoid-like. As with delta-9-THC, tolerance develops rapidly to the pharmacological effects in both the dog and the monkey. Cross-tolerance between Cesamet and delta-9-THC was demonstrated in the monkey.
Dependence—The physical dependence capacity of Cesamet is unknown at this time. Patients who participated in clinical trials of up to 5 days’ duration evidenced no withdrawal symptoms on cessation of dosing.
Overdosage
Signs and Symptoms—Signs and symptoms of overdosage are an extension of the psychotomimetic and physiologic effects of Cesamet.
Treatment—To obtain up-to-date information about the treatment of overdose, a good resource is your certified Regional Poison Control Center. Telephone numbers of certified poison control centers are uled in the Physicians’ Desk Reference (PDR). In managing overdosage, consider the possibility of multiple drug overdoses, interaction among drugs, and unusual drug kinetics in your patient.
Overdosage may be considered to have occurred, even at prescribed dosages, if disturbing psychiatric symptoms are present. In these cases, the patient should be observed in a quiet environment and supportive measures, including reassurance, should be used. Subsequent doses should be withheld until patients have returned to their baseline mental status; routine dosing may then be resumed if clinically indicated. In such instances, a lower initiating dose is suggested. In controlled clinical trials, alterations in mental status related to the use of Cesamet resolved within 72 hours without specific medical therapy.
In overdose settings, attention should be paid to vital signs, since both hypertension and hypotension have been known to occur; tachycardia and orthostatic hypotension were most commonly reported.
No cases of overdosage with more than 10 mg/day of nabilone were reported during clinical trials. Signs and symptoms that would be expected to occur in large overdose situations are psychotic episodes, including hallucinations, anxiety reactions, respiratory depression, and coma.
If psychotic episodes occur, the patient should be managed conservatively, if possible. For moderate psychotic episodes and anxiety reactions, verbal support and comforting may be sufficient. In more severe cases, antipsychotic drugs may be useful; however, the utility of antipsychotic drugs in cannabinoid psychosis has not been systematically evaluated. Support for their use is drawn from limited experience using antipsychotic agents to manage cannabis overdoses. Because of the potential for drug-drug interactions (e.g., additive CNS depressant effects due to nabilone and chlorpromazine), such patients should be closely monitored.
Protect the patient’s airway and support ventilation and perfusion. Meticulously monitor and maintain, within acceptable limits, the patient’s vital signs, blood gases, serum electrolytes, as well as other laboratory values and physical assessments. Absorption of drugs from the gastrointestinal tract may be decreased by giving activated charcoal, which, in many cases, is more effective than emesis or lavage; consider charcoal instead of or in addition to gastric emptying. Repeated doses of charcoal over time may hasten elimination of some drugs that have been absorbed. Safeguard the patient’s airway when employing gastric emptying or charcoal.
The use of forced diuresis, peritoneal dialysis, hemodialysis, charcoal hemoperfusion, or cholestyramine has not been reported. In the presence of normal renal function, most of a dose of nabilone is eliminated through the biliary system.
Treatment for respiratory depression and comatose state consists in symptomatic and supportive therapy. Particular attention should be paid to the occurrence of hypothermia. If the patient becomes hypotensive, consider fluids, inotropes, and/or vasopressors.
The estimated oral median lethal dose in female mice is between 1,000 and 2,000 mg/kg; in the female rat, it is greater than 2,000 mg/kg (see CLINICAL PHARMACOLOGY ).
Dosage And Administration
The usual adult dosage is 1 or 2 mg 2 times a day. On the day of chemotherapy, the initial dose should be given 1 to 3 hours before the chemotherapeutic agent is administered. To minimize side effects, it is recommended that the lower starting dose be used and that the dose be increased as necessary. A dose of 1 or 2 mg the night before may be useful. The maximum recommended daily dose is 6 mg given in divided doses 3 times a day.
Cesamet may be administered 2 or 3 times a day during the entire course of each cycle of chemotherapy and, if needed, for 48 hours after the last dose of each cycle of chemotherapy.
How Supplied
Cesamet® capsules (blue and white): 1 mg (bottles of 50 capsules) NDC 0187-1231-50. Capsules are imprinted with ICN on the blue cap and a four-digit code (3101) on the white body. Store at controlled room temperature 25°C (77°F); excursions permitted to 15° to 30°C (59° to 86°F) [see USP Controlled Room Temperature].
Distributed by:
Bausch Health US, LLCBridgewater, NJ 08807 USA
Manufactured by: Bausch Health Companies Inc.Laval, Quebec H7L 4A8, Canada
Cesamet is a trademark of Bausch Health Companies Inc. or its affiliates.
© 2021 Bausch Health Companies Inc. or its affiliates
9754700 Rev. 02/2021
Package/label Principal Display Panel
NDC 0187-1231-50 Rx Only
Cesamet® CII (nabilone) capsules   1 mg
50 Capsules
Each capsule contains 1 mg nabilone
BAUSCH Health
DISCLAIMER:
"This tool does not provide medical advice, and is for informational and educational purposes only, and is not a substitute for professional medical advice, treatment or diagnosis. Call your doctor to receive medical advice. If you think you may have a medical emergency, please dial 911."
"Do not rely on openFDA to make decisions regarding medical care. While we make every effort to ensure that data is accurate, you should assume all results are unvalidated. We may limit or otherwise restrict your access to the API in line with our Terms of Service."
"This product uses publicly available data from the U.S. National Library of Medicine (NLM), National Institutes of Health, Department of Health and Human Services; NLM is not responsible for the product and does not endorse or recommend this or any other product."
PillSync may earn a commission via links on our site
