Clorazepate Dipotassium Dailymed
Generic: clorazepate dipotassium is used for the treatment of Alcohol Withdrawal Delirium Anxiety Disorders Epilepsies, Partial Glaucoma, Angle-Closure


Go PRO for all pill images
CIV
Rx only
Description
Chemically, clorazepate dipotassium is a benzodiazepine. The empirical formula is C16H11ClK2N2O4; the molecular weight is 408.92; 1H-1, 4-Benzodiazepine-3-carboxylic acid, 7-chloro-2,3-dihydro-2-oxo-5-phenyl-, potassium salt compound with potassium hydroxide (1:1) and the structural formula may be represented as follows:
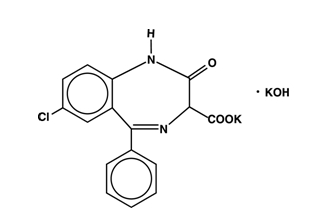
The compound occurs as a fine, light yellow, practically odorless powder. It is insoluble in the common organic solvents, but very soluble in water. Aqueous solutions are unstable, clear, light yellow, and alkaline
Clorazepate Dipotassium Tablets, USP for oral administration, contain 3.75 mg, 7.5 mg or 15 mg of clorazepate dipotassium, USP. In addition, each tablet contains the following inactive ingredients: croscarmellose sodium, magnesium oxide, magnesium stearate, microcrystalline cellulose, potassium carbonate, sodium chloride, sodium lauryl sulfate and the following coloring agents:
3.75 mg - FD&C Blue No. 2 Aluminum Lake
7.5 mg - FD&C Yellow No. 6 Aluminum Lake
Clinical Pharmacology
Pharmacologically, clorazepate dipotassium has the characteristics of the benzodiazepines. It has depressant effects on the central nervous system. The primary metabolite, nordiazepam, quickly appears in the blood stream. The serum half-life is about 2 days. The drug is metabolized in the liver and excreted primarily in the urine. Studies in healthy men have shown that clorazepate dipotassium has depressant effects on the central nervous system. Prolonged administration of single daily doses as high as 120 mg was without toxic effects. Abrupt cessation of high doses was followed in some patients by nervousness, insomnia, irritability, diarrhea, muscle aches, or memory impairment.
Since orally administered clorazepate dipotassium is rapidly decarboxylated to form nordiazepam, there is essentially no circulating parent drug. Nordiazepam, the primary metabolite, quickly appears in the blood and is eliminated from the plasma with an apparent half-life of about 40 to 50 hours. Plasma levels of nordiazepam increase proportionally with Clorazepate Dipotassium dose and show moderate accumulation with repeated administration. The protein binding of nordiazepam in plasma is high (97-98%).
Within 10 days after oral administration of a 15 mg (50µCi) dose of 14C-Clorazepate Dipotassium to two volunteers, 62-67% of the radioactivity was excreted in the urine and 15-19% was eliminated in the feces. Both subjects were still excreting measurable amounts of radioactivity in the urine (about l% of the 14C-dose) on day ten.
Nordiazepam is further metabolized by hydroxylation. The major urinary metabolite is conjugated oxazepam (3-hydroxynordiazepam), and smaller amounts of conjugated p-hydroxynordiazepam and nordiazepam are also found in the urine.
Indications And Usage
Clorazepate dipotassium is indicated for the management of anxiety disorders or for the short-term relief of the symptoms of anxiety. Anxiety or tension associated with the stress of everyday life usually does not require treatment with an anxiolytic.
Clorazepate dipotassium tablets are indicated as adjunctive therapy in the management of partial seizures.
The effectiveness of clorazepate dipotassium tablets in long-term management of anxiety, that is, more than 4 months, has not been assessed by systematic clinical studies. Long-term studies in epileptic patients, however, have shown continued therapeutic activity. The physician should reassess periodically the usefulness of the drug for the individual patient.
Clorazepate dipotassium tablets are indicated for the symptomatic relief of acute alcohol withdrawal.
Contraindications
Clorazepate dipotassium tablets are contraindicated in patients with a known hypersensitivity to the drug and in those with acute narrow angle glaucoma.
Warnings
Clorazepate dipotassium tablets are not recommended for use in depressive neuroses or in psychotic reactions.
Patients taking clorazepate dipotassium tablets should be cautioned against engaging in hazardous occupations requiring mental alertness, such as operating dangerous machinery including motor vehicles.
Since clorazepate dipotassium has a central nervous system depressant effect, patients should be advised against the simultaneous use of other CNS-depressant drugs, and cautioned that the effects of alcohol may be increased.
Because of the lack of sufficient clinical experience, clorazepate dipotassium tablets are not recommended for use in patients less than 9 years of age.
Physical and Psychological Dependence
Withdrawal symptoms (similar in character to those noted with barbiturates and alcohol) have occurred following abrupt discontinuance of clorazepate. Withdrawal symptoms associated with the abrupt discontinuation of benzodiazepines have included convulsions, delirium, tremor, abdominal and muscle cramps, vomiting, sweating, nervousness, insomnia, irritability, diarrhea, and memory impairment. The more severe withdrawal symptoms have usually been limited to those patients who had received excessive doses over an extended period of time. Generally milder withdrawal symptoms have been reported following abrupt discontinuance of benzodiazepines taken continuously at therapeutic levels for several months. Consequently, after extended therapy, abrupt discontinuation of clorazepate should generally be avoided and a gradual dosage tapering schedule followed.
Caution should be observed in patients who are considered to have a psychological potential for drug dependence.
Evidence of drug dependence has been observed in dogs and rabbits which was characterized by convulsive seizures when the drug was abruptly withdrawn or the dose was reduced; the syndrome in dogs could be abolished by administration of clorazepate.
Usage in Pregnancy
An increased risk of congenital malformations associated with the use of minor tranquilizers (chlordiazepoxide, diazepam, and meprobamate) during the first trimester of pregnancy has been suggested in several studies. Clorazepate dipotassium, a benzodiazepine derivative, has not been studied adequately to determine whether it, too, may be associated with an increased risk of fetal abnormality. Because use of these drugs is rarely a matter of urgency, their use during this period should almost always be avoided. The possibility that a woman of childbearing potential may be pregnant at the time of institution of therapy should be considered. Patients should be advised that if they become pregnant during therapy or intend to become pregnant they should communicate with their physician about the desirability of discontinuing the drug.
Usage during Lactation
Clorazepate dipotassium tablets should not be given to nursing mothers since it has been reported that nordiazepam is excreted in human breast milk.
Precautions
In those patients in which a degree of depression accompanies the anxiety, suicidal tendencies may be present and protective measures may be required. The least amount of drug that is feasible should be available to the patient.
Patients taking clorazepate dipotassium tablets for prolonged periods should have blood counts and liver function tests periodically. The usual precautions in treating patients with impaired renal or hepatic function should also be observed.
In elderly or debilitated patients, the initial dose should be small, and increments should be made gradually, in accordance with the response of the patient to preclude ataxia or excessive sedation.
Information for Patients
To assure the safe and effective use of benzodiazepines, patients should be informed that, since benzodiazepines may produce psychological and physical dependence, it is essential that they consult with their physician before either increasing the dose or abruptly discontinuing this drug.
Pediatric Use
See WARNINGS.
Geriatric Use
Clinical studies of clorazepate dipotassium studies were not adequate to determine whether subjects aged 65 and over respond differently than younger subjects. Elderly or debilitated patients may be especially sensitive to the effects of all benzodiazepines, including clorazepate dipotassium. In general, elderly or debilitated patients should be started on lower doses of clorazepate dipotassium tablets and observed closely, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and concomitant disease or other drug therapy. Dose adjustments should also be made slowly, and with more caution in this patient population (see PRECAUTIONS and DOSAGE AND ADMINISTRATION).
Adverse Reactions
The side effect most frequently reported was drowsiness. Less commonly reported (in descending order of occurrence) were: dizziness, various gastrointestinal complaints, nervousness, blurred vision, dry mouth, headache, and mental confusion. Other side effects included insomnia, transient skin rashes, fatigue, ataxia, genitourinary complaints, irritability, diplopia, depression, tremor and slurred speech.
There have been reports of abnormal liver and kidney function tests and of decrease in hematocrit.
Decrease in systolic blood pressure has been observed.
Dosage And Administration
For the symptomatic relief of anxiety
Clorazepate dipotassium tablets are administered orally in divided doses. The usual daily dose is 30 mg. The dose should be adjusted gradually within the range of 15 to 60 mg daily in accordance with the response of the patient. In elderly or debilitated patients it is advisable to initiate treatment at a daily dose of 7.5 to 15 mg.
Clorazepate dipotassium tablets may also be administered in a single dose daily at bedtime; the recommended initial dose is 15 mg. After the initial dose, the response of the patient may require adjustment of subsequent dosage. Lower doses may be indicated in the elderly patient. Drowsiness may occur at the initiation of treatment and with dosage increment.
For the symptomatic relief of acute alcohol withdrawal
The following dosage schedule is recommended
1st 24 hours(Day 1) 30 mg initially, followed by 30 to 60 mg in divided doses 2nd 24 hours(Day 2) 45 to 90 mg in divided doses 3rd 24 hours(Day 3) 22.5 to 45 mg in divided doses Day 4 15 to 30 mg in divided doses
Thereafter, gradually reduce the daily dose to 7.5 to 15 mg. Discontinue drug therapy as soon as patient's condition is stable.
The maximum recommended total daily dose is 90 mg. Avoid excessive reductions in the total amount of drug administered on successive days.
As an Adjunct to Antiepileptic Drugs
In order to minimize drowsiness, the recommended initial dosages and dosage increments should not be exceeded.
Adults
The maximum recommended initial dose in patients over 12 years old is 7.5 mg three times a day. Dosage should be increased by no more than 7.5 mg every week and should not exceed 90 mg/day.
Children (9-12 years)
The maximum recommended initial dose is 7.5 mg two times a day. Dosage should be increased by no more than 7.5 mg every week and should not exceed 60 mg/day.
Drug Interactions
If clorazepate dipotassium is to be combined with other drugs acting on the central nervous system, careful consideration should be given to the pharmacology of the agents to be employed. Animal experience indicates that clorazepate dipotassium prolongs the sleeping time after hexobarbital or after ethyl alcohol, increases the inhibitory effects of chlorpromazine, but does not exhibit monoamine oxidase inhibition. Clinical studies have shown increased sedation with concurrent hypnotic medications. The actions of the benzodiazepines may be potentiated by barbiturates, narcotics, phenothiazines, monoamine oxidase inhibitors or other antidepressants.
If clorazepate dipotassium tablets are used to treat anxiety associated with somatic disease states, careful attention must be paid to possible drug interaction with concomitant medication.
In bioavailability studies with normal subjects, the concurrent administration of antacids at therapeutic levels did not significantly influence the bioavailability of clorazepate dipotassium tablets.
Overdosage
Overdosage is usually manifested by varying degrees of CNS depression ranging from slight sedation to coma. As in the management of overdosage with any drug, it should be borne in mind that multiple agents may have been taken.
The treatment of overdosage should consist of the general measures employed in the management of overdosage of any CNS depressant. Gastric evacuation either by the induction of emesis, lavage, or both, should be performed immediately. General supportive care, including frequent monitoring of the vital signs and close observation of the patient is indicated. Hypotension though rarely reported, may occur with large overdoses. In such cases the use of agents such as Levophed® Bitartrate (norepinephrine bitartrate injection, USP) or Aramine® Injection metaraminol bitartrate injection, USP) should be considered.
While reports indicate that individuals have survived overdoses of clorazepate dipotassium as high as 450 to 675 mg, these doses are not necessarily an accurate indication of the amount of drug absorbed since the time interval between ingestion and the institution of treatment was not always known. Sedation in varying degrees was the most common physiological manifestation of clorazepate dipotassium overdosage. Deep coma when it occurred was usually associated with the ingestion of other drugs in addition to clorazepate dipotassium.
Flumazenil, a specific benzodiazepine receptor antagonist, is indicated for the complete or partial reversal of the sedative effects of benzodiazepines and may be used in situations when an overdose with a benzodiazepine is known or suspected. Prior to the administration of flumazenil, necessary measures should be instituted to secure airway, ventilation, and intravenous access. Flumazenil is intended as an adjunct to, not as a substitute for, proper management of benzodiazepine overdose. Patients treated with flumazenil should be monitored for resedation, respiratory depression, and other residual benzodiazepine effects for an appropriate period after treatment. The prescriber should be aware of a risk of seizure in association with flumazenil treatment, particularly in long-term benzodiazepine users and in cyclic antidepressant overdose. The complete flumazenil package insert including CONTRAINDICATIONS, WARNINGS, and PRECAUTIONS should be consulted prior to use
Animal Pharmacology And Toxicology
Studies in rats and monkeys have shown a substantial difference between doses producing tranquilizing, sedative and toxic effects. In rats, conditioned avoidance response was inhibited at an oral dose of 10 mg/kg; sedation was induced at 32 mg/kg; the LD50 was 1320 mg/kg. In monkeys aggressive behavior was reduced at an oral dose of 0.25 mg/kg; sedation (ataxia) was induced at 7.5 mg/kg; the LD50 could not be determined because of the emetic effect of large doses, but the LD50 exceeds 1600 mg/kg.
Twenty-four dogs were given clorazepate dipotassium orally in a 22-month toxicity study; doses up to 75 mg/kg were given. Drug-related changes occurred in the liver; weight was increased and cholestasis with minimal hepatocellular damage was found, but lobular architecture remained well preserved.
Eighteen rhesus monkeys were given oral doses of clorazepate dipotassium from 3 to 36 mg/kg daily for 52 weeks. All treated animals remained similar to control animals. Although total leucocyte count remained within normal limits it tended to fall in the female animals on the highest doses.
Examination of all organs revealed no alterations attributable to clorazepate dipotassium. There was no damage to liver function or structure.
Reproduction Studies
Standard fertility, reproduction, and teratology studies were conducted in rats and rabbits. Oral doses in rats up to 150 mg/kg and in rabbits up to 15 mg/kg produced no abnormalities in the fetuses. Clorazepate dipotassium did not alter the fertility indices or reproductive capacity of adult animals. As expected, the sedative effect of high doses interfered with care of the young by their mothers (see Usage in Pregnancy ).
How Supplied
The 7.5 mg tablets are peach round, scored tablets debossed with M above the score and 40 below the score on one side of the tablet and blank on the other side. They are available as follows:
NDC 67046-906-30buler of 30 tablets
Recommended storage
Protect from moisture. Keep bottle tightly closed. Store between 20° to 25°C (68° to 70°F) [see USP Controlled Room temperature]. Dispense in a USP tight, light-resistant container.
Mylan Pharmaceuticals Inc.Morgantown, WV 26505
Repackaged by: Contract Pharmacy Services-PA125 Titus Ave Suite 200Warrington, PA 18976 USA
Original--3/2011--NJW
Principal Display Panel
7.5 mg Tablets
DISCLAIMER:
"This tool does not provide medical advice, and is for informational and educational purposes only, and is not a substitute for professional medical advice, treatment or diagnosis. Call your doctor to receive medical advice. If you think you may have a medical emergency, please dial 911."
"Do not rely on openFDA to make decisions regarding medical care. While we make every effort to ensure that data is accurate, you should assume all results are unvalidated. We may limit or otherwise restrict your access to the API in line with our Terms of Service."
"This product uses publicly available data from the U.S. National Library of Medicine (NLM), National Institutes of Health, Department of Health and Human Services; NLM is not responsible for the product and does not endorse or recommend this or any other product."
PillSync may earn a commission via links on our site
