Harvoni (ledipasvir 90 mg sofosbuvir 400 mg) Dailymed
Generic: ledipasvir and sofosbuvir is used for the treatment of Hepatitis C, Chronic Hemoglobinopathies Pregnancy Hepatitis, Autoimmune Renal Insufficiency

IMPRINT: GSI 7985
SHAPE: diamond
COLOR: orange
Boxed Warning
Warning: Risk Of Hepatitis B Virus Reactivation In Patients Coinfected With Hcv And Hbv

Go PRO for all pill images
Warning: Risk Of Hepatitis B Virus Reactivation In Patients Coinfected With Hcv And Hbv
Test all patients for evidence of current or prior hepatitis B virus (HBV) infection before initiating treatment with HARVONI. HBV reactivation has been reported in HCV/HBV coinfected patients who were undergoing or had completed treatment with HCV direct acting antivirals and were not receiving HBV antiviral therapy. Some cases have resulted in fulminant hepatitis, hepatic failure, and death. Monitor HCV/HBV coinfected patients for hepatitis flare or HBV reactivation during HCV treatment and post-treatment follow-up. Initiate appropriate patient management for HBV infection as clinically indicated [see Warnings and Precautions (5.1)].
WARNING: RISK OF HEPATITIS B VIRUS REACTIVATION IN PATIENTS COINFECTED WITH HCV AND HBV
See full prescribing information for complete boxed warning.
Hepatitis B virus (HBV) reactivation has been reported, in some cases resulting in fulminant hepatitis, hepatic failure, and death. (5.1 )
Recent Major Changes Section
Indications and Usage ( 1 )8/2019 Dosage and Administration   Recommended Treatment Regimen and Duration in Patients 3 Years of Age and Older with Genotype 1, 4, 5, or 6 HCV ( 2.2 )8/2019   Recommended Dosage in Pediatric Patients 3 Years of Age and Older ( 2.4 )8/2019   Preparation and Administration of Oral Pellets ( 2.5 )8/2019   Renal Impairment ( 2.6 )11/2019
1 Indications And Usage
HARVONI is indicated for the treatment of adults and pediatric patients 3 years of age and older with chronic hepatitis C virus (HCV) [see Dosage and Administration (2.2 and 2.3) and Clinical Studies (14)]:
- genotype 1, 4, 5, or 6 infection without cirrhosis or with compensated cirrhosis
- genotype 1 infection with decompensated cirrhosis, for use in combination with ribavirin
- genotype 1 or 4 infection who are liver transplant recipients without cirrhosis or with compensated cirrhosis, for use in combination with ribavirin
HARVONI is a fixed-dose combination of ledipasvir, a hepatitis C virus (HCV) NS5A inhibitor, and sofosbuvir, an HCV nucleotide analog NS5B polymerase inhibitor, and is indicated for the treatment of chronic hepatitis C virus (HCV) in adults and pediatric patients 3 years of age and older:
- Genotype 1, 4, 5, or 6 infection without cirrhosis or with compensated cirrhosis
- Genotype 1 infection with decompensated cirrhosis, in combination with ribavirin
- Genotype 1 or 4 infection who are liver transplant recipients without cirrhosis or with compensated cirrhosis, in combination with ribavirin. (
1 )
2 Dosage And Administration
- Testing prior to the initiation of therapy: Test all patients for HBV infection by measuring HBsAg and anti-HBc. (
2.1 )- Recommended treatment regimen and duration in patients 3 years of age and older: (
2.2 )
HCV Genotype Patient Population Regimen and Duration Genotype 1 Treatment-na√Įve without cirrhosis or with compensated cirrhosis (Child-Pugh A) HARVONI 12 weeks Treatment-experienced without cirrhosis HARVONI 12 weeks Treatment-experienced with compensated cirrhosis (Child-Pugh A) HARVONI 24 weeks Treatment-na√Įve and treatment-experienced with decompensated cirrhosis (Child-Pugh B or C) HARVONI + ribavirin 12 weeks Genotype 1 or 4 Treatment-na√Įve and treatment-experienced liver transplant recipients without cirrhosis, or with compensated cirrhosis (Child-Pugh A) HARVONI + ribavirin 12 weeks Genotype 4, 5, or 6 Treatment-na√Įve and treatment-experienced without cirrhosis or with compensated cirrhosis (Child-Pugh A) HARVONI 12 weeks
- Recommended dosage in adults: One tablet (90 mg of ledipasvir and 400 mg of sofosbuvir) taken orally once daily with or without food. (
2.3 )- Recommended dosage in pediatric patients 3 years and older: Recommended dosage of HARVONI in pediatric patients 3 years of age and older is based on weight. Refer to Table 2 of the full prescribing information for specific dosing guidelines based on body weight. (
2.4 )- Instructions for Use should be followed for preparation and administration of HARVONI oral pellets. (
2.5 )- HCV/HIV-1 coinfection: For adult and pediatric patients with HCV/HIV-1 coinfection, follow the dosage recommendations in the tables in the full prescribing information. (
2.3 ,2.4 )- If used in combination with ribavirin, follow the recommendations for ribavirin dosing and dosage modifications. (
2.3 ,2.4 )- For patients with any degree of renal impairment, including end stage renal disease on dialysis, no HARVONI dosage adjustment is recommended. (
2.6 )2.1 Testing Prior to the Initiation of Therapy
Test all patients for evidence of current or prior HBV infection by measuring hepatitis B surface antigen (HBsAg) and hepatitis B core antibody (anti-HBc) before initiating HCV treatment with HARVONI [see Warnings and Precautions (5.1)].
2.2Recommended Treatment Regimen and Duration in Patients 3 Years of Age and Older with Genotype 1, 4, 5, or 6 HCV
Table 1 shows the recommended HARVONI treatment regimen and duration based on patient population. Relapse rates are affected by baseline host and viral factors and differ between treatment durations for certain subgroups [see Clinical Studies (14)].
For patients with HCV/HIV-1 coinfection, follow the dosage recommendations in Table 1 [see Clinical Studies (14)]. Refer to Drug Interactions (7) for dosage recommendations for concomitant HIV-1 antiviral drugs.
Table 1 Recommended Treatment Regimen and Duration for HARVONI in Patients 3 Years of Age and Older with Genotype 1, 4, 5, or 6 HCV HCV Genotype Patient Population Treatment Regimen and Duration Genotype 1 Treatment-na√Įve without cirrhosis or with compensated cirrhosis (Child-Pugh A) HARVONI 12 weeks HARVONI for 8 weeks can be considered in treatment-na√Įve genotype 1 patients without cirrhosis who have pretreatment HCV RNA less than 6 million IU/mL [see Clinical Studies (14.2)]. Treatment-experienced Treatment-experienced adult and pediatric subjects have failed a peginterferon alfa +/- ribavirin based regimen with or without an HCV protease inhibitor. without cirrhosisHARVONI 12 weeks Treatment-experienced with compensated cirrhosis (Child-Pugh A) HARVONI 24 weeks HARVONI + ribavirin for 12 weeks can be considered in treatment-experienced genotype 1 patients with cirrhosis who are eligible for ribavirin [see Dosage and Administration (2.3 and 2.4) and Clinical Studies (14.2)]. Treatment-na√Įve and treatment-experienced with decompensated cirrhosis (Child-Pugh B or C) HARVONI + ribavirin See Dosage and Administration 2.3 and 2.4 for ribavirin dosage recommendations. 12 weeksGenotype 1 or 4 Treatment-na√Įve and treatment-experienced liver transplant recipients without cirrhosis, or with compensated cirrhosis (Child-Pugh A) HARVONI + ribavirin 12 weeks Genotype 4, 5, or 6 Treatment-na√Įve and treatment-experienced , without cirrhosis or with compensated cirrhosis (Child-Pugh A) HARVONI 12 weeks 2.3Recommended Dosage in Adults
The recommended dosage of HARVONI in adults with genotype 1, 4, 5, or 6 HCV is one tablet (90 mg ledipasvir and 400 mg sofosbuvir) taken orally once daily with or without food [see Clinical Pharmacology (12.3)].
The daily dosage of ribavirin is weight-based (1000 mg for patients <75 kg and 1200 mg for those ‚Č•75 kg) administered orally in two divided doses with food.
In patients with decompensated cirrhosis, the starting dosage of ribavirin is 600 mg and can be titrated up to 1000 mg for patients <75 kg and 1200 mg for those ‚Č•75 kg in two divided doses with food. If the starting dosage of ribavirin is not well tolerated, the dosage should be reduced as clinically indicated based on hemoglobin levels.
For further information on ribavirin dosing and dosage modifications, refer to the ribavirin prescribing information [see Dosage and Administration (2.4), Use in Specific Populations (8.6), and Clinical Studies (14.5)].
2.4Recommended Dosage in Pediatric Patients 3 Years of Age and Older
The recommended dosage of HARVONI in pediatric patients 3 years of age and older with genotype 1, 4, 5, or 6 HCV using HARVONI tablets or oral pellets is based on weight (Table 2). Table 3 provides the weight-based dosage of ribavirin when used in combination with HARVONI for pediatric patients. Take HARVONI tablets or pellets (with or without food) once daily [see Dosage and Administration (2.5), Clinical Pharmacology (12.3), and Clinical Studies (14.7)]. HARVONI pellets can be taken in pediatric patients who cannot swallow the tablet formulation.
Table 2 Dosing for Pediatric Patients 3 Years and Older Using HARVONI Tablets or Oral Pellets Body Weight (kg) Dosing of HARVONI Tablets or Oral Pellets HARVONI Daily Dose at least 35 one 90 mg/400 mg tablet once daily or two 45 mg/200 mg tablets once daily or two 45 mg/200 mg packets of pellets once daily 90 mg/400 mg per day 17 to less than 35 one 45 mg/200 mg tablet once daily or one 45 mg/200 mg packet of pellets once daily 45 mg/200 mg per day less than17 one 33.75 mg/150 mg packet of pellets once daily 33.75 mg/150 mg per day
Table 3 Recommended Dosing for Ribavirin in Combination Therapy with HARVONI for Pediatric Patients 3 Years and Older Body Weight (kg) Oral Ribavirin Daily Dosage The daily dosage of ribavirin is weight-based and is administered orally in two divided doses with food. less than 47 15 mg per kg per day (divided dose AM and PM) 47‚Äď49 600 mg per day (1 √ó 200 mg AM, 2 √ó 200 mg PM) 50‚Äď65 800 mg per day (2 √ó 200 mg AM, 2 √ó 200 mg PM) 66‚Äď80 1000 mg per day (2 √ó 200 mg AM, 3 √ó 200 mg PM) greater than 80 1200 mg per day (3 √ó 200 mg AM, 3 √ó 200 mg PM) 2.5Preparation and Administration of Oral Pellets
See the HARVONI oral pellets full Instructions for Use for details on the preparation and administration of HARVONI pellets.
Do not chew HARVONI pellets. If HARVONI pellets are administered with food, sprinkle the pellets on one or more spoonfuls of non-acidic soft food at or below room temperature. Examples of non-acidic foods include pudding, chocolate syrup, mashed potato, and ice cream. Take HARVONI pellets within 30 minutes of gently mixing with food and swallow the entire contents without chewing to avoid a bitter aftertaste.
2.6 Renal Impairment
No dosage adjustment of HARVONI is recommended in patients with any degree of renal impairment, including end stage renal disease (ESRD) on dialysis [see Dosage and Administration (2.3)]. Take HARVONI with or without ribavirin according to the recommendations in Table 1 [see Adverse Reactions (6.1), Use in Specific Populations (8.6), and Clinical Studies (14.6)]. Refer to ribavirin tablet prescribing information for ribavirin dosage modification for patients with CrCl less than or equal to 50 mL per minute.
3 Dosage Forms And Strengths
HARVONI is available as tablets or pellets for oral use. Each dosage form is available in two dose strengths.
- 90 mg/400 mg Tablets: orange, diamond-shaped, film-coated tablet debossed with "GSI" on one side and "7985" on the other side of the tablet. Each tablet contains 90 mg ledipasvir and 400 mg sofosbuvir.
- 45 mg/200 mg Tablets: white, capsule-shaped, film-coated tablets, debossed with "GSI" on one side and "HRV" on the other side. Each tablet contains 45 mg ledipasvir and 200 mg sofosbuvir.
- 45 mg/200 mg Pellets: orange pellets in unit-dose packets. Each packet contains 45 mg ledipasvir and 200 mg sofosbuvir.
- 33.75 mg/150 mg Pellets: orange pellets in unit-dose packets. Each packet contains 33.75 mg ledipasvir and 150 mg sofosbuvir.
- Tablets: 90 mg of ledipasvir and 400 mg of sofosbuvir; 45 mg of ledipasvir and 200 mg of sofosbuvir. (
3 )- Oral Pellets: 45 mg of ledipasvir and 200 mg of sofosbuvir; 33.75 mg of ledipasvir and 150 mg of sofosbuvir. (
3 )
4 Contraindications
If HARVONI is administered with ribavirin, the contraindications to ribavirin also apply to this combination regimen. Refer to the ribavirin prescribing information for a ul of contraindications for ribavirin [see Dosage and Administration (2.2)].
If used in combination with ribavirin, all contraindications to ribavirin also apply to HARVONI combination therapy. (4 )
5 Warnings And Precautions
- Risk of Hepatitis B Virus Reactivation: Test all patients for evidence of current or prior HBV infection before initiation of HCV treatment. Monitor HCV/HBV coinfected patients for HBV reactivation and hepatitis flare during HCV treatment and post-treatment follow-up. Initiate appropriate patient management for HBV infection as clinically indicated. (
5.1 )- Bradycardia with amiodarone coadministration: Serious symptomatic bradycardia may occur in patients taking amiodarone, particularly in patients also receiving beta blockers, or those with underlying cardiac comorbidities and/or advanced liver disease. Coadministration of amiodarone with HARVONI is not recommended. In patients without alternative, viable treatment options, cardiac monitoring is recommended. (
5.2 ,6.2 ,7.2 )5.1Risk of Hepatitis B Virus Reactivation in Patients Coinfected with HCV and HBV
Hepatitis B virus (HBV) reactivation has been reported in HCV/HBV coinfected patients who were undergoing or had completed treatment with HCV direct acting antivirals, and who were not receiving HBV antiviral therapy. Some cases have resulted in fulminant hepatitis, hepatic failure, and death. Cases have been reported in patients who are HBsAg positive and also in patients with serologic evidence of resolved HBV infection (i.e., HBsAg negative and anti-HBc positive). HBV reactivation has also been reported in patients receiving certain immunosuppressants or chemotherapeutic agents; the risk of HBV reactivation associated with treatment with HCV direct-acting antivirals may be increased in these patients.
HBV reactivation is characterized as an abrupt increase in HBV replication manifesting as a rapid increase in serum HBV DNA level. In patients with resolved HBV infection, reappearance of HBsAg can occur. Reactivation of HBV replication may be accompanied by hepatitis, i.e., increases in aminotransferase levels and, in severe cases, increases in bilirubin levels, liver failure, and death can occur.
Test all patients for evidence of current or prior HBV infection by measuring HBsAg and anti-HBc before initiating HCV treatment with HARVONI. In patients with serologic evidence of HBV infection, monitor for clinical and laboratory signs of hepatitis flare or HBV reactivation during HCV treatment with HARVONI and during post-treatment follow-up. Initiate appropriate patient management for HBV infection as clinically indicated.
5.2Serious Symptomatic Bradycardia When Coadministered with Amiodarone
Postmarketing cases of symptomatic bradycardia, as well as fatal cardiac arrest and cases requiring pacemaker intervention, have been reported when amiodarone is coadministered with HARVONI. Bradycardia has generally occurred within hours to days, but cases have been observed up to 2 weeks after initiating HCV treatment. Patients also taking beta blockers, or those with underlying cardiac comorbidities and/or advanced liver disease, may be at increased risk for symptomatic bradycardia with coadministration of amiodarone. Bradycardia generally resolved after discontinuation of HCV treatment. The mechanism for this effect is unknown.
Coadministration of amiodarone with HARVONI is not recommended. For patients taking amiodarone who have no other alternative, viable treatment options and who will be coadministered HARVONI:
- Counsel patients about the risk of serious symptomatic bradycardia
- Cardiac monitoring in an in-patient setting for the first 48 hours of coadministration is recommended, after which outpatient or self-monitoring of the heart rate should occur on a daily basis through at least the first 2 weeks of treatment.
Patients who are taking HARVONI who need to start amiodarone therapy due to no other alternative, viable treatment options should undergo similar cardiac monitoring as outlined above.
Due to amiodarone's long half-life, patients discontinuing amiodarone just prior to starting HARVONI should also undergo similar cardiac monitoring as outlined above.
Patients who develop signs or symptoms of bradycardia should seek medical evaluation immediately. Symptoms may include near-fainting or fainting, dizziness or lightheadedness, malaise, weakness, excessive tiredness, shortness of breath, chest pains, confusion, or memory problems [see Adverse Reactions (6.2), Drug Interactions (7.2)].
5.3 Risk of Reduced Therapeutic Effect Due to Use with P-gp Inducers
The concomitant use of HARVONI and P-gp inducers may significantly decrease ledipasvir and sofosbuvir plasma concentrations and may lead to a reduced therapeutic effect of HARVONI. Therefore, the use of HARVONI with P-gp inducers (e.g., rifampin, St. John's wort) is not recommended [see Drug Interactions (7.2)].
5.4Risks Associated with Ribavirin Combination Treatment
If HARVONI is administered with ribavirin, the warnings and precautions for ribavirin, in particular the pregnancy avoidance warning, apply to this combination regimen. Refer to the ribavirin prescribing information for a full ul of the warnings and precautions for ribavirin [see Dosage and Administration (2.2)].
6 Adverse Reactions
The following serious adverse reactions are described below and elsewhere in labeling:
- Serious Symptomatic Bradycardia When Coadministered with Amiodarone [see Warnings and Precautions (5.2)].
- The most common adverse reactions (incidence greater than or equal to 10%, all grades) observed with treatment with HARVONI were fatigue, headache, and asthenia. (
6.1 )
To report SUSPECTED ADVERSE REACTIONS, contact Gilead Sciences, Inc. at 1-800-GILEAD-5 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
6.1Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
If HARVONI is administered with ribavirin to adults, refer to the prescribing information for ribavirin for a description of ribavirin-associated adverse reactions.
Clinical Trials in Adult Subjects
The safety assessment of HARVONI was based on pooled data from three randomized, open-label Phase 3 clinical trials (ION-3, ION-1, and ION-2) of subjects with genotype 1 HCV with compensated liver disease (with and without cirrhosis) including 215, 539, and 326 subjects who received HARVONI once daily by mouth for 8, 12, and 24 weeks, respectively [see Clinical Studies (14)].
The proportion of subjects who permanently discontinued treatment due to adverse events was 0%, less than 1%, and 1% for subjects receiving HARVONI for 8, 12, and 24 weeks, respectively.
The most common adverse reactions (at least 10%) were fatigue and headache in subjects treated with 8, 12, or 24 weeks of HARVONI.
Table 4 uls adverse reactions (adverse events assessed as causally related by the investigator, all grades) observed in at least 5% of subjects receiving 8, 12, or 24 weeks of treatment with HARVONI in clinical trials. The majority of adverse reactions presented in Table 4 occurred at severity of grade 1. The side-by-side tabulation is to simplify presentation; direct comparison across trials should not be made due to differing trial designs.
Table 4 Adverse Reactions (All Grades) Reported in ‚Č•5% of Subjects Receiving 8, 12, or 24 Weeks of Treatment with HARVONI HARVONI 8 weeks (N=215) HARVONI 12 weeks (N=539) HARVONI 24 weeks (N=326) Fatigue 16% 13% 18% Headache 11% 14% 17% Nausea 6% 7% 9% Diarrhea 4% 3% 7% Insomnia 3% 5% 6%
The safety assessment of HARVONI was also based on pooled data from three open-label trials (Study 1119, ION-4, and ELECTRON-2) in 118 subjects with chronic HCV genotype 4, 5, or 6 infection with compensated liver disease (with or without cirrhosis) [see Clinical Studies (14.3)]. The subjects received HARVONI once daily by mouth for 12 weeks. The safety profile in subjects with chronic HCV genotype 4, 5, or 6 infection with compensated liver disease was similar to that observed in subjects with chronic HCV genotype 1 infection with compensated liver disease. The most common adverse reactions occurring in at least 10% of subjects were asthenia (18%), headache (14%), and fatigue (10%).
Adverse Reactions in Subjects with Cirrhosis
The safety assessment of HARVONI with or without ribavirin was based on a randomized, double-blind and placebo-controlled trial in treatment-experienced genotype 1 subjects with compensated cirrhosis and was compared to placebo in the SIRIUS trial. Subjects were randomized to receive 24 weeks of HARVONI once daily by mouth without ribavirin or 12 weeks of placebo followed by 12 weeks of HARVONI once daily by mouth + ribavirin [see Clinical Studies (14.2)]. Table 5 presents the adverse reactions, as defined above, that occurred with at least 5% greater frequency in subjects treated with 24 weeks of HARVONI or 12 weeks of HARVONI + ribavirin, compared to those reported for 12 weeks of placebo. The majority of the adverse reactions presented in Table 5 were Grade 1 or 2 in severity.
Table 5 Adverse Reactions with ‚Č•5% Greater Frequency Reported in Treatment-Experienced Subjects with Cirrhosis Receiving HARVONI for 24 Weeks or HARVONI + Ribavirin for 12 Weeks Compared to Placebo for 12 weeks HARVONI 24 weeks (N=78) HARVONI + RBV 12 weeks (N=76) Placebo 12 weeks (N=77) RBV=ribavirin Asthenia 31% 36% 23% Headache 29% 13% 16% Fatigue 18% 4% 1% Cough 5% 11% 1% Myalgia 9% 4% 0 Dyspnea 3% 9% 1% Irritability 8% 7% 1% Dizziness 5% 1% 0
Adverse Reactions in Subjects Coinfected with HIV-1
The safety assessment of HARVONI was based on an open-label clinical trial in 335 genotype 1 or 4 subjects with HCV/HIV-1 coinfection who were on stable antiretroviral therapy in Study ION-4 [see Clinical Studies (14.4)]. The safety profile in HCV/HIV-1 coinfected subjects was similar to that observed in HCV mono-infected subjects. The most common adverse reactions occurring in at least 10% of subjects were headache (20%) and fatigue (17%).
Adverse Reactions in Liver Transplant Recipients and/or Subjects with Decompensated Cirrhosis
The safety assessment of HARVONI with ribavirin in liver transplant recipients and/or those who had decompensated liver disease was based on pooled data from two Phase 2 open-label clinical trials including 336 subjects who received HARVONI plus ribavirin for 12 weeks. Subjects with Child-Pugh-Turcotte (CPT) scores greater than 12 were excluded from the trials [see Clinical Studies (14.5)].
The adverse events observed were consistent with the expected clinical sequelae of liver transplantation and/or decompensated liver disease, or the known safety profile of HARVONI and/or ribavirin.
Decreases in hemoglobin to less than 10 g/dL and 8.5 g/dL during treatment were observed in 38% and 13% of subjects treated with HARVONI plus ribavirin for 12 weeks, respectively. Ribavirin was permanently discontinued in 11% of subjects treated with HARVONI plus ribavirin for 12 weeks.
Liver Transplant Recipients with Compensated Liver Disease:
Among the 174 liver transplant recipients with compensated liver disease who received HARVONI with ribavirin for 12 weeks, 2 (1%) subjects permanently discontinued HARVONI due to an adverse event.
Subjects with Decompensated Liver Disease:
Among the 162 subjects with decompensated liver disease (pre- or post-transplant) who received HARVONI with ribavirin for 12 weeks, 7 (4%) subjects died, 4 (2%) subjects underwent liver transplantation, and 1 subject (<1%) underwent liver transplantation and died during treatment or within 30 days after discontinuation of treatment. Because these events occurred in patients with advanced liver disease who are at risk of progression of liver disease including liver failure and death, it is not possible to reliably assess the contribution of drug effect to outcomes. A total of 4 (2%) subjects permanently discontinued HARVONI due to an adverse event.
Less Common Adverse Reactions Reported in Clinical Trials (less than 5%): The following adverse reactions occurred in less than 5% of subjects receiving HARVONI in any one trial. These events have been included because of their seriousness or assessment of potential causal relationship.
Psychiatric disorders: depression (including in subjects with pre-existing history of psychiatric illness).
Depression (particularly in subjects with pre-existing history of psychiatric illness) occurred in subjects receiving sofosbuvir containing regimens. Suicidal ideation and suicide have occurred in less than 1% of subjects treated with sofosbuvir in combination with ribavirin or pegylated interferon/ribavirin in other clinical trials.
Laboratory Abnormalities
Bilirubin Elevations: Bilirubin elevations of greater than 1.5√óULN were observed in 3%, less than 1%, and 2% of subjects treated with HARVONI for 8, 12, and 24 weeks, respectively. Bilirubin elevations of greater than 1.5√óULN were observed in 3%, 11%, and 3% of subjects with compensated cirrhosis treated with placebo, HARVONI + ribavirin for 12 weeks, and HARVONI for 24 weeks, respectively, in the SIRIUS trial.
Lipase Elevations: Transient, asymptomatic lipase elevations of greater than 3√óULN were observed in less than 1%, 2%, and 3% of subjects treated with HARVONI for 8, 12, and 24 weeks, respectively. Transient, asymptomatic lipase elevations of greater than 3√ó ULN were observed in 1%, 3%, and 9% of subjects with compensated cirrhosis treated with placebo, HARVONI + ribavirin for 12 weeks, and HARVONI for 24 weeks, respectively, in the SIRIUS trial.
Creatine Kinase: Creatine kinase was not assessed in Phase 3 trials ION-3, ION-1, or ION-2 of HARVONI. Creatine kinase was assessed in the ION-4 trial. Isolated, asymptomatic creatine kinase elevations of greater than or equal to 10√óULN was observed in 1% of subjects treated with HARVONI for 12 weeks in the ION-4 trial and has also been previously reported in subjects treated with sofosbuvir in combination with ribavirin or peginterferon/ribavirin in other clinical trials.
Adverse Reactions in Adults with Severe Renal Impairment, Including those on Dialysis
In an open-label trial (Trial 0154) in which adults with HCV with compensated liver disease (with or without cirrhosis) and severe renal impairment received HARVONI for 12 weeks (N=18), the most common adverse reaction was fatigue (17%) [see Clinical Studies (14.6)].
In an open-label clinical trial, Trial 4063, a total of 95 adults with HCV with compensated liver disease (with or without cirrhosis) and ESRD requiring dialysis received HARVONI for 8 (n=45), 12 (n=31), or 24 (n=19) weeks. The most common adverse reactions were insomnia and headache (each reported in 4% of subjects overall) [see Clinical Studies (14.6)].
Adverse Reactions in Pediatric Subjects 3 Years of Age and Older
The safety assessment of HARVONI in pediatric subjects 3 years of age and older is based on data from a Phase 2, open-label clinical trial (Study 1116). In total, 226 subjects were enrolled, which included 223 subjects without cirrhosis or with compensated cirrhosis who were treated with HARVONI for 12 weeks; one genotype 1 treatment-experienced subject with cirrhosis who was treated with HARVONI for 24 weeks; and two genotype 3 subjects who were treated with HARVONI + ribavirin for 24 weeks. The adverse reactions observed were consistent with those observed in clinical studies of HARVONI in adults. Limited safety data are available in pediatric subjects receiving HARVONI for 24 weeks. No Grade 3 or 4 adverse reactions or discontinuation due to an adverse reaction was observed in those pediatric subjects receiving HARVONI for 24 weeks [see Clinical Studies (14.7)].
6.2Postmarketing Experience
The following adverse reactions have been identified during post approval use of HARVONI. Because postmarketing reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Cardiac Disorders
Serious symptomatic bradycardia has been reported in patients taking amiodarone who initiate treatment with HARVONI [see Warnings and Precautions (5.2), Drug Interactions (7.2)].
Skin and Subcutaneous Tissue Disorders
Skin rashes, sometimes with bulers or angioedema-like swelling
Angioedema
7 Drug Interactions
- Coadministration with amiodarone may result in serious symptomatic bradycardia. Use of HARVONI with amiodarone is not recommended. (
5.2 ,6.2 ,7.2 )- P-gp inducers (e.g., rifampin, St. John's wort): May alter concentrations of ledipasvir and sofosbuvir. Use of HARVONI with P-gp inducers is not recommended. (
5.3 ,7 ,12.3 )- Consult the full prescribing information prior to use for potential drug interactions. (
5.2 ,5.3 ,7 ,12.3 )- Clearance of HCV infection with direct acting antivirals may lead to changes in hepatic function, which may impact safe and effective use of concomitant medications. Frequent monitoring of relevant laboratory parameters (INR or blood glucose) and dose adjustments of certain concomitant medications may be necessary. (
7.2 )7.1Potential for Drug Interaction
As HARVONI contains ledipasvir and sofosbuvir, any interactions that have been identified with these agents individually may occur with HARVONI.
After oral administration of HARVONI, sofosbuvir is rapidly absorbed and subject to extensive first-pass hepatic extraction. In clinical pharmacology studies, both sofosbuvir and the inactive metabolite GS-331007 were monitored for purposes of pharmacokinetic analyses.
Ledipasvir is an inhibitor of the drug transporters P-gp and breast cancer resistance protein (BCRP) and may increase intestinal absorption of coadministered substrates for these transporters.
Ledipasvir and sofosbuvir are substrates of drug transporters P-gp and BCRP while GS-331007 is not. P-gp inducers (e.g., rifampin, St. John's wort) may decrease ledipasvir and sofosbuvir plasma concentrations, leading to reduced therapeutic effect of HARVONI, and the use with P-gp inducers is not recommended with HARVONI [see Warnings and Precautions (5.3)].
7.2Established and Potentially Significant Drug Interactions
Clearance of HCV infection with direct acting antivirals may lead to changes in hepatic function, which may impact the safe and effective use of concomitant medications. For example, altered blood glucose control resulting in serious symptomatic hypoglycemia has been reported in diabetic patients in postmarketing case reports and published epidemiological studies. Management of hypoglycemia in these cases required either discontinuation or dose modification of concomitant medications used for diabetes treatment.
Frequent monitoring of relevant laboratory parameters (e.g., International Normalized Ratio [INR] in patients taking warfarin, blood glucose levels in diabetic patients) or drug concentrations of concomitant medications such as cytochrome P450 substrates with a narrow therapeutic index (e.g., certain immunosuppressants) is recommended to ensure safe and effective use. Dose adjustments of concomitant medications may be necessary.
Table 6 provides a uling of established or potentially clinically significant drug interactions. The drug interactions described are based on studies conducted with either HARVONI, the components of HARVONI (ledipasvir and sofosbuvir) as individual agents, or are predicted drug interactions that may occur with HARVONI [see Warnings and Precautions (5.2, 5.3) and Clinical Pharmacology (12.3)].
Table 6 Potentially Significant Drug Interactions: Alteration in Dose or Regimen May Be Recommended Based on Drug Interaction Studies or Predicted Interaction This table is not all inclusive. Concomitant Drug Class: Drug Name Effect on Concentration ‚Üď = decrease, ‚ÜĎ = increase Clinical Comment tenofovir DF = tenofovir disoproxil fumarate Acid Reducing Agents: ‚Üď ledipasvir Ledipasvir solubility decreases as pH increases. Drugs that increase gastric pH are expected to decrease concentration of ledipasvir. Antacids (e.g., aluminum and magnesium hydroxide) It is recommended to separate antacid and HARVONI administration by 4 hours. H2-receptor antagonists These interactions have been studied in healthy adults. (e.g., famotidine)H2-receptor antagonists may be administered simultaneously with or 12 hours apart from HARVONI at a dose that does not exceed doses comparable to famotidine 40 mg twice daily. Proton-pump inhibitors (e.g., omeprazole) Proton-pump inhibitor doses comparable to omeprazole 20 mg or lower can be administered simultaneously with HARVONI under fasted conditions. Antiarrhythmics: amiodarone Effect on amiodarone, ledipasvir, and sofosbuvir concentrations unknown Coadministration of amiodarone with HARVONI may result in serious symptomatic bradycardia. The mechanism of this effect is unknown. Coadministration of amiodarone with HARVONI is not recommended; if coadministration is required, cardiac monitoring is recommended [see Warnings and Precautions (5.2), Adverse Reactions (6.2)]. digoxin ‚ÜĎ digoxin Coadministration of HARVONI with digoxin may increase the concentration of digoxin. Therapeutic concentration monitoring of digoxin is recommended when coadministered with HARVONI. Anticonvulsants: carbamazepine phenytoin phenobarbital ‚Üď ledipasvir ‚Üď sofosbuvir Coadministration of HARVONI with carbamazepine, phenytoin, or phenobarbital is expected to decrease the concentration of ledipasvir and sofosbuvir, leading to reduced therapeutic effect of HARVONI. Coadministration is not recommended. Antimycobacterials: rifabutin rifampin rifapentine ‚Üď ledipasvir ‚Üď sofosbuvir Coadministration of HARVONI with rifampin, rifabutin, or rifapentine is not recommended [see Warnings and Precautions (5.3)]. HIV Antiretrovirals: Regimens containing tenofovir DF without an HIV protease inhibitor/ ritonavir or cobicistat ‚ÜĎ tenofovir Monitor for tenofovir-associated adverse reactions in patients receiving HARVONI concomitantly with a regimen containing tenofovir DF without an HIV protease inhibitor/ritonavir or cobicistat. Refer to VIREAD or TRUVADA prescribing information for recommendations on renal monitoring. Regimens containing tenofovir DF and an HIV protease inhibitor/ ritonavir or cobicistat
- atazanavir/ritonavir or cobicistat + emtricitabine/tenofovir DF
- darunavir/ritonavir or cobicistat + emtricitabine/tenofovir DF
- lopinavir/ritonavir + emtricitabine/tenofovir DF
‚ÜĎ tenofovir The safety of increased tenofovir concentrations in the setting of HARVONI and an HIV protease inhibitor/ritonavir or cobicistat has not been established. Consider alternative HCV or antiretroviral therapy to avoid increases in tenofovir exposures. If coadministration is necessary, monitor for tenofovir-associated adverse reactions. Refer to VIREAD or TRUVADA prescribing information for recommendations on renal monitoring. elvitegravir, cobicistat, emtricitabine, tenofovir DF ‚ÜĎ tenofovir The safety of increased tenofovir concentrations in the setting of HARVONI and the combination of elvitegravir, cobicistat, emtricitabine, and tenofovir DF has not been established. Coadministration is not recommended. tipranavir/ritonavir ‚Üď ledipasvir ‚Üď sofosbuvir Coadministration of HARVONI with tipranavir/ritonavir is expected to decrease the concentration of ledipasvir and sofosbuvir, leading to reduced therapeutic effect of HARVONI. Coadministration is not recommended. HCV Products: simeprevir ‚ÜĎ ledipasvir ‚ÜĎ simeprevir Concentrations of ledipasvir and simeprevir are increased when simeprevir is coadministered with ledipasvir. Coadministration of HARVONI with simeprevir is not recommended. Herbal Supplements: St. John's wort (Hypericum perforatum) ‚Üď ledipasvir ‚Üď sofosbuvir Coadministration of HARVONI with St. John's wort, a P-gp inducer, is not recommended [see Warnings and Precautions (5.3)]. HMG-CoA Reductase Inhibitors: rosuvastatin ‚ÜĎ rosuvastatin Coadministration of HARVONI with rosuvastatin may significantly increase the concentration of rosuvastatin, which is associated with increased risk of myopathy, including rhabdomyolysis. Coadministration of HARVONI with rosuvastatin is not recommended. atorvastatin ‚ÜĎ atorvastatin Coadministration of HARVONI with atorvastatin may be associated with increased risk of myopathy, including rhabdomyolysis. Monitor closely for HMG-CoA reductase inhibitor-associated adverse reactions, such as myopathy and rhabdomyolysis. 7.3Drugs without Clinically Significant Interactions with HARVONI
Based on drug interaction studies conducted with the components of HARVONI (ledipasvir or sofosbuvir) or HARVONI, no clinically significant drug interactions have been either observed or are expected when HARVONI is used with the following drugs [see Clinical Pharmacology (12.3)]: abacavir, atazanavir/ritonavir, cyclosporine, darunavir/ritonavir, dolutegravir, efavirenz, elvitegravir/cobicistat/emtricitabine/tenofovir alafenamide, emtricitabine, lamivudine, methadone, midazolam, oral contraceptives, pravastatin, raltegravir, rilpivirine, tacrolimus, or verapamil. See Table 6 for use of HARVONI with certain HIV antiretroviral regimens [see Drug Interactions (7.2)].
8 Use In Specific Populations
- Pediatric Use: No data are available regarding the safety of HARVONI in pediatric patients with renal impairment. (
8.4 )8.1 Pregnancy
Risk Summary
If HARVONI is administered with ribavirin, the combination regimen is contraindicated in pregnant women and in men whose female partners are pregnant. Refer to the ribavirin prescribing information for more information on ribavirin-associated risks of use during pregnancy.
No adequate human data are available to establish whether or not HARVONI poses a risk to pregnancy outcomes. In animal reproduction studies, no evidence of adverse developmental outcomes was observed with the components of HARVONI (ledipasvir or sofosbuvir) at exposures greater than those in humans at the recommended human dose (RHD) [see Data]. During organogenesis in the rat and rabbit, systemic exposures (AUC) to ledipasvir were approximately 4 (rats) and 2 (rabbits) times the exposure in humans at the RHD, while exposures to the predominant circulating metabolite of sofosbuvir (GS-331007) were ‚Č•3 (rats) and 7 (rabbits) times the exposure in humans at the RHD. In rat pre/postnatal development studies, maternal systemic exposures (AUC) to ledipasvir and GS-331007 were approximately 5 and 7 times, respectively, the exposure in humans at the RHD.
The background risk of major birth defects and miscarriage for the indicated population is unknown. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2‚Äď4% and 15‚Äď20%, respectively.
Data
Animal Data
8.2 Lactation
Risk Summary
It is not known whether ledipasvir or sofosbuvir, the components of HARVONI, or their metabolites are present in human breast milk, affect human milk production or have effects on the breastfed infant. When administered to lactating rats, ledipasvir was detected in the plasma of nursing pups likely due to the presence of ledipasvir in milk, without clear effects on nursing pups [see Data]. The predominant circulating metabolite of sofosbuvir (GS-331007) was the primary component observed in the milk of lactating rats, without effect on nursing pups.
The development and health benefits of breastfeeding should be considered along with the mother's clinical need for HARVONI and any potential adverse effects on the breastfed child from HARVONI or from the underlying maternal condition.
If HARVONI is administered with ribavirin, the nursing mother's information for ribavirin also applies to this combination regimen. Refer to the ribavirin prescribing information for more information on use during lactation.
Data
Ledipasvir: No effects of ledipasvir on growth and postnatal development were observed in nursing pups at the highest dose tested in rats. Maternal systemic exposure (AUC) to ledipasvir was approximately 5 times the exposure in humans at the RHD. Although not measured directly, ledipasvir was likely present in the milk of lactating rats, since systemic exposure (AUC) to ledipasvir of approximately 25% that of maternal exposure was observed in nursing pups on lactation day 10.
Sofosbuvir: No effects of sofosbuvir on growth and postnatal development were observed in nursing pups at the highest dose tested in rats. Maternal systemic exposure (AUC) to the predominant circulating metabolite of sofosbuvir (GS-331007) was approximately 7 times the exposure in humans at the RHD, with exposure of approximately 2% that of maternal exposure observed in nursing pups on lactation day 10. In a lactation study, sofosbuvir metabolites (primarily GS-331007) were excreted into the milk of lactating rats following administration of a single oral dose of sofosbuvir (20 mg/kg) on lactation day 2, with milk concentrations of approximately 10% that of maternal plasma concentrations observed 1 hour post-dose.
8.3 Females and Males of Reproductive Potential
If HARVONI is administered with ribavirin, the information for ribavirin with regard to pregnancy testing, contraception, and infertility also applies to this combination regimen. Refer to ribavirin prescribing information for additional information.
8.4 Pediatric Use
The safety, pharmacokinetics, and efficacy of HARVONI for treatment of HCV genotype 1 and 4 infection in treatment-na√Įve and treatment-experienced pediatric patients 3 years of age and older without cirrhosis or with compensated cirrhosis have been established in an open-label, multicenter clinical trial (Study 1116, N=226; 186 treatment-na√Įve, 40 treatment-experienced) and are comparable to that observed in adults.
The safety and efficacy of HARVONI for treatment of HCV genotypes 5 or 6 infection in pediatric patients 3 years of age and older are supported by comparable ledipasvir, sofosbuvir, and GS-331007 exposures between adults and pediatric patients [see Dosage and Administration (2.2 and 2.4), Adverse Reactions (6.1), Clinical Pharmacology (12.3), and Clinical Studies (14.3, 14.6, 14.7)]. Similar rationale is used to support dosing recommendations for pediatric patients with HCV genotype 1 infection who have decompensated cirrhosis (Child-Pugh B or C) and for pediatric patients with HCV genotype 1 and 4 infection who are liver transplant recipients without cirrhosis or with compensated cirrhosis.
In patients with severe renal impairment, including those requiring dialysis, exposures of GS-331007, the inactive metabolite of sofosbuvir, are increased [see Clinical Pharmacology (12.3)]. No data are available regarding the safety of HARVONI in pediatric patients with renal impairment [see Use in Specific Populations (8.6)].
The safety and efficacy of HARVONI have not been established in pediatric patients less than 3 years of age.
8.5 Geriatric Use
Clinical trials of HARVONI included 225 subjects aged 65 and over (9% of total number of subjects in the clinical studies). No overall differences in safety or effectiveness were observed between these subjects and younger subjects, and other reported clinical experience has not identified differences in responses between the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out. No dosage adjustment of HARVONI is warranted in geriatric patients [see Clinical Pharmacology (12.3)].
8.6Renal Impairment
No dosage adjustment of HARVONI is recommended for patients with mild, moderate, or severe renal impairment, including ESRD requiring dialysis [see Dosage and Administration (2.4), Adverse Reactions (6.1), Clinical Pharmacology (12.3), and Clinical Studies (14.6)]. No safety data are available in subjects with both decompensated cirrhosis and severe renal impairment, including those on dialysis. Additionally, no safety data are available in pediatric patients with renal impairment [see Use in Specific Populations (8.4)]. Refer to ribavirin tablet prescribing information regarding use in patients with renal impairment.
8.7Hepatic Impairment
No dosage adjustment of HARVONI is recommended for patients with mild, moderate, or severe hepatic impairment (Child-Pugh Class A, B, or C) [see Dosage and Administration (2.3), Clinical Pharmacology (12.3) and Clinical Studies (14.5)].
Clinical and hepatic laboratory monitoring, as clinically indicated, is recommended for patients with decompensated cirrhosis receiving treatment with HARVONI and ribavirin [see Adverse Reactions (6.1)].
10 Overdosage
No specific antidote is available for overdose with HARVONI. If overdose occurs, the patient must be monitored for evidence of toxicity. Treatment of overdose with HARVONI consists of general supportive measures including monitoring of vital signs as well as observation of the clinical status of the patient. Hemodialysis is unlikely to result in significant removal of ledipasvir since ledipasvir is highly bound to plasma protein. Hemodialysis can efficiently remove the predominant circulating metabolite of sofosbuvir, GS-331007, with an extraction ratio of 53%.
11 Description
Tablets
HARVONI tablets are fixed-dose combination tablets containing ledipasvir and sofosbuvir for oral administration. Ledipasvir is an HCV NS5A inhibitor and sofosbuvir is a nucleotide analog inhibitor of HCV NS5B polymerase.
Each 90 mg/400 mg tablet contains 90 mg ledipasvir and 400 mg sofosbuvir. The tablets include the following inactive ingredients: colloidal silicon dioxide, copovidone, croscarmellose sodium, lactose monohydrate, magnesium stearate, and microcrystalline cellulose. The tablets are film-coated with a coating material containing the following inactive ingredients: FD&C yellow #6/sunset yellow FCF aluminum lake, polyethylene glycol, polyvinyl alcohol, talc, and titanium dioxide.
Each 45 mg/200 mg tablet contains 45 mg ledipasvir and 200 mg sofosbuvir. The tablets include the following inactive ingredients: colloidal silicon dioxide, copovidone, croscarmellose sodium, lactose monohydrate, magnesium stearate, and microcrystalline cellulose. The tablets are film-coated with a coating material containing the following inactive ingredients: polyethylene glycol, polyvinyl alcohol, talc, and titanium dioxide.
Pellets
HARVONI oral pellets are for oral administration, supplied as small, orange pellets in unit-dose packets. Each unit-dose of HARVONI oral pellets contains either 45 mg ledipasvir and 200 mg sofosbuvir or 33.75 mg ledipasvir and 150 mg sofosbuvir and the following inactive ingredients: amino-methacrylate copolymer, colloidal silicon dioxide, copovidone, croscarmellose sodium, hypromellose, lactose monohydrate, iron oxide red, iron oxide yellow, magnesium stearate, microcrystalline cellulose, polyethylene glycol, talc, and titanium dioxide.
Ledipasvir: The IUPAC name for ledipasvir is methyl [(2S)-1-{(6S)-6-[5-(9,9-difluoro-7-{2-[(1R,3S,4S)-2-{(2S)-2-[(methoxycarbonyl)amino]-3-methylbutanoyl}-2-azabicyclo[2.2.1]hept-3-yl]-1H-benzimidazol-6-yl}-9H-fluoren-2-yl)-1H-imidazol-2-yl]-5-azaspiro[2.4]hept-5-yl}-3-methyl-1-oxobutan-2-yl]carbamate.
It has a molecular formula of C49H54F2N8O6 and a molecular weight of 889.00. It has the following structural formula:
Ledipasvir is practically insoluble (less than 0.1 mg/mL) across the pH range of 3.0‚Äď7.5 and is slightly soluble below pH 2.3 (1.1 mg/mL).
Sofosbuvir: The IUPAC name for sofosbuvir is (S)-isopropyl 2-((S)-(((2R,3R,4R,5R)-5-(2,4-dioxo-3,4-dihydropyrimidin-1(2H)-yl)-4-fluoro-3-hydroxy-4-methyltetrahydrofuran-2-yl)methoxy)-(phenoxy)phosphorylamino)propanoate. It has a molecular formula of C22H29FN3O9P and a molecular weight of 529.45. It has the following structural formula:
Sofosbuvir is a white to off-white crystalline solid with a solubility of at least 2 mg/mL across the pH range of 2‚Äď7.7 at 37¬įC and is slightly soluble in water.
12 Clinical Pharmacology
12.1 Mechanism of Action
HARVONI is a fixed-dose combination of ledipasvir and sofosbuvir, which are direct-acting antiviral agents against the hepatitis C virus [see Microbiology (12.4)].
12.2 Pharmacodynamics
Cardiac Electrophysiology
Thorough QT studies have been conducted for ledipasvir and sofosbuvir.
The effect of ledipasvir 120 mg twice daily (2.67 times the maximum recommended dosage) for 10 days on QTc interval was evaluated in a randomized, multiple-dose, placebo-, and active-controlled (moxifloxacin 400 mg) three-period crossover thorough QT trial in 59 healthy subjects. At the dose of 120 mg twice daily (2.67 times the maximum recommended dosage), ledipasvir does not prolong QTc interval to any clinically relevant extent.
The effect of sofosbuvir 400 mg (maximum recommended dosage) and 1200 mg (three times the maximum recommended dosage) on QTc interval was evaluated in a randomized, single-dose, placebo-, and active-controlled (moxifloxacin 400 mg) four-period crossover thorough QT trial in 59 healthy subjects. At a dose three times the maximum recommended dose, sofosbuvir does not prolong QTc to any clinically relevant extent.
12.3 Pharmacokinetics
Absorption
The pharmacokinetic properties of ledipasvir, sofosbuvir, and the predominant circulating metabolite GS-331007 have been evaluated in healthy adult subjects and in subjects with chronic hepatitis C. Following oral administration of HARVONI, ledipasvir median peak concentrations were observed 4 to 4.5 hours post-dose. Sofosbuvir was absorbed quickly and the peak median plasma concentration was observed ~0.8 to 1 hour post-dose. Median peak plasma concentration of GS-331007 was observed between 3.5 to 4 hours post-dose.
Based on the population pharmacokinetic analysis in HCV-infected subjects, geometric mean steady-state AUC0‚Äď24 for ledipasvir (N=2113), sofosbuvir (N=1542), and GS-331007 (N=2113) were 7290, 1320, and 12,000 ng‚ąôhr/mL, respectively. Steady-state Cmax for ledipasvir, sofosbuvir, and GS-331007 were 323, 618, and 707 ng/mL, respectively. Sofosbuvir and GS-331007 AUC0‚Äď24 and Cmax were similar in healthy adult subjects and subjects with HCV infection. Relative to healthy subjects (N=191), ledipasvir AUC0‚Äď24 and Cmax were 24% lower and 32% lower, respectively, in HCV-infected subjects.
Effect of Food
Relative to fasting conditions, the administration of a single dose of HARVONI with a moderate fat (~600 kcal, 25% to 30% fat) or high fat (~1000 kcal, 50% fat) meal increased sofosbuvir AUC0‚Äďinf by approximately 2-fold, but did not significantly affect sofosbuvir Cmax. The exposures of GS-331007 and ledipasvir were not altered in the presence of either meal type. The response rates in Phase 3 trials were similar in HCV-infected subjects who received HARVONI with food or without food. HARVONI can be administered without regard to food.
Distribution
Ledipasvir is greater than 99.8% bound to human plasma proteins. After a single 90 mg dose of [14C]-ledipasvir in healthy subjects, the blood to plasma ratio of 14C-radioactivity ranged between 0.51 and 0.66.
Sofosbuvir is approximately 61‚Äď65% bound to human plasma proteins and the binding is independent of drug concentration over the range of 1 microgram/mL to 20 microgram/mL. Protein binding of GS-331007 was minimal in human plasma. After a single 400 mg dose of [14C]-sofosbuvir in healthy subjects, the blood to plasma ratio of 14C-radioactivity was approximately 0.7.
Metabolism
In vitro, no detectable metabolism of ledipasvir was observed by human CYP1A2, CYP2C8, CYP2C9, CYP2C19, CYP2D6, and CYP3A4. Evidence of slow oxidative metabolism via an unknown mechanism has been observed. Following a single dose of 90 mg [14C]-ledipasvir, systemic exposure was almost exclusively to the parent drug (greater than 98%). Unchanged ledipasvir is the major species present in feces.
Sofosbuvir is extensively metabolized in the liver to form the pharmacologically active nucleoside analog triphosphate GS-461203. The metabolic activation pathway involves sequential hydrolysis of the carboxyl ester moiety catalyzed by human cathepsin A (CatA) or carboxylesterase 1 (CES1) and phosphoramidate cleavage by histidine triad nucleotide-binding protein 1 (HINT1) followed by phosphorylation by the pyrimidine nucleotide biosynthesis pathway. Dephosphorylation results in the formation of nucleoside metabolite GS-331007 that cannot be efficiently rephosphorylated and lacks anti-HCV activity in vitro. After a single 400 mg oral dose of [14C]-sofosbuvir, GS-331007 accounted for approximately greater than 90% of total systemic exposure.
Elimination
Following a single 90 mg oral dose of [14C]-ledipasvir, mean total recovery of the [14C]-radioactivity in feces and urine was approximately 87%, with most of the radioactive dose recovered from feces (approximately 86%). Unchanged ledipasvir excreted in feces accounted for a mean of 70% of the administered dose and the oxidative metabolite M19 accounted for 2.2% of the dose. These data indicate that biliary excretion of unchanged ledipasvir is a major route of elimination, with renal excretion being a minor pathway (approximately 1%). The median terminal half-life of ledipasvir following administration of HARVONI was 47 hours.
Following a single 400 mg oral dose of [14C]-sofosbuvir, mean total recovery of the dose was greater than 92%, consisting of approximately 80%, 14%, and 2.5% recovered in urine, feces, and expired air, respectively. The majority of the sofosbuvir dose recovered in urine was GS-331007 (78%) while 3.5% was recovered as sofosbuvir. These data indicate that renal clearance is the major elimination pathway for GS-331007. The median terminal half-lives of sofosbuvir and GS-331007 following administration of HARVONI were 0.5 and 27 hours, respectively.
Specific Populations
Race: Population pharmacokinetics analysis in HCV-infected subjects indicated that race had no clinically relevant effect on the exposure of ledipasvir, sofosbuvir, and GS-331007.
Gender: Population pharmacokinetics analysis in HCV-infected subjects indicated that gender had no clinically relevant effect on the exposure of sofosbuvir and GS-331007. AUC and Cmax of ledipasvir were 77% and 58% higher, respectively, in females than males; however, the relationship between gender and ledipasvir exposures was not considered clinically relevant, as high response rates (SVR12 >90%) were achieved in male and female subjects across the Phase 3 studies and the safety profiles are similar in females and males.
Pediatric Patients: The pharmacokinetics of ledipasvir, sofosbuvir, and GS-331007 were determined in HCV genotype 1, 3, or 4 infected pediatric subjects 3 years of age and older receiving a daily dose of HARVONI as described below in Table 7. Exposures in pediatric subjects were similar to those observed in adults.
Table 7 Pharmacokinetic Properties of the Components of HARVONI in HCV-Infected Pediatric Subjects 3 Years of Age and Older Population PK derived parameters Weight Group Dose PK Parameter Geometric Mean (%CV) Ledipasvir Sofosbuvir GS-331007 ‚Č•35 kg Ledipasvir N=100; Sofosbuvir N=72; GS-331007 N=100 90/400 mg AUCtau (ng‚ąôhr/mL) 11200 (45.7) 1350 (45.2) 13600 (18.9) Cmax (ng/mL) 550 (44.2) 660 (51.1) 921 (17.8) 17 to <35 kg Ledipasvir N=86; Sofosbuvir N=66; GS-331007 N=86 45/200 mg AUCtau (ng‚ąôhr/mL) 8750 (46.6) 1420 (34.2) 10700 (30.9) Cmax (ng/mL) 440 (42.7) 690 (24.8) 958 (26.1) <17 kg Ledipasvir N=9; Sofosbuvir N=9; GS-331007 N=9 33.75/150 mg AUCtau (ng‚ąôhr/mL) 7460 (31.0) 1720 (23.2) 12200 (15.2) Cmax (ng/mL) 405 (25.7) 791 (16.6) 1070 (13.0)
The pharmacokinetics of ledipasvir, sofosbuvir, and GS-331007 have not been established in pediatric subjects less than 3 years of age [see Use in Specific Populations (8.4) and Clinical Studies (14.7)].
Geriatric Patients: Population pharmacokinetic analysis in HCV-infected subjects showed that within the age range (18 to 80 years) analyzed, age did not have a clinically relevant effect on the exposure to ledipasvir, sofosbuvir, and GS-331007 [see Use in Specific Populations (8.5)].
Patients with Renal Impairment: The pharmacokinetics of ledipasvir were studied with a single dose of 90 mg ledipasvir in HCV negative subjects with severe renal impairment (eGFR less than 30 mL/min by Cockcroft-Gault). No clinically relevant differences in ledipasvir pharmacokinetics were observed between healthy subjects and subjects with severe renal impairment.
The pharmacokinetics of sofosbuvir were studied in HCV negative subjects with mild (eGFR between 50 to less than 80 mL/min/1.73 m2), moderate (eGFR between 30 to less than 50 mL/min/1.73 m2), severe renal impairment (eGFR less than 30 mL/min/1.73 m2), and subjects with ESRD requiring hemodialysis following a single 400 mg dose of sofosbuvir. Relative to subjects with normal renal function (eGFR greater than 80 mL/min/1.73 m2), the sofosbuvir AUC0‚Äďinf was 61%, 107%, and 171% higher in mild, moderate, and severe renal impairment, while the GS-331007 AUC0‚Äďinf was 55%, 88%, and 451% higher, respectively. In subjects with ESRD, relative to subjects with normal renal function, sofosbuvir and GS-331007 AUC0‚Äďinf was 28% and 1280% higher when sofosbuvir was dosed 1 hour before hemodialysis compared with 60% and 2070% higher when sofosbuvir was dosed 1 hour after hemodialysis, respectively. A 4-hour hemodialysis session removed approximately 18% of administered dose [see Dosage and Administration (2.6) and Use in Specific Populations (8.6)].
The pharmacokinetics of ledipasvir, sofosbuvir, and GS-331007 were studied in HCV-infected subjects with severe renal impairment or ESRD requiring dialysis treated with HARVONI for 8, 12, or 24 weeks. The results were generally consistent with those observed in HCV-negative subjects with ESRD requiring dialysis.
Patients with Hepatic Impairment: The pharmacokinetics of ledipasvir were studied with a single dose of 90 mg ledipasvir in HCV negative subjects with severe hepatic impairment (Child-Pugh Class C). Ledipasvir plasma exposure (AUC0‚Äďinf) was similar in subjects with severe hepatic impairment and control subjects with normal hepatic function. Population pharmacokinetics analysis in HCV-infected subjects indicated that cirrhosis (including decompensated cirrhosis) had no clinically relevant effect on the exposure of ledipasvir [see Use in Specific Populations (8.7)].
The pharmacokinetics of sofosbuvir were studied following 7-day dosing of 400 mg sofosbuvir in HCV-infected subjects with moderate and severe hepatic impairment (Child-Pugh Class B and C). Relative to subjects with normal hepatic function, the sofosbuvir AUC0‚Äď24 were 126% and 143% higher in moderate and severe hepatic impairment, while the GS-331007 AUC0‚Äď24 were 18% and 9% higher, respectively. Population pharmacokinetics analysis in HCV-infected subjects indicated that cirrhosis (including decompensated cirrhosis) had no clinically relevant effect on the exposure of sofosbuvir and GS-331007 [see Use in Specific Populations (8.7) and Clinical Studies (14.5)].
Drug Interaction Studies
Ledipasvir and sofosbuvir are substrates of drug transporters P-gp and BCRP while GS-331007 is not. P-gp inducers (e.g., rifampin or St. John's wort) may decrease ledipasvir and sofosbuvir plasma concentrations, leading to reduced therapeutic effect of HARVONI, and the use with P-gp inducers is not recommended with HARVONI [see Warnings and Precautions (5.3)]. Coadministration with drugs that inhibit P-gp and/or BCRP may increase ledipasvir and sofosbuvir plasma concentrations without increasing GS-331007 plasma concentration; HARVONI may be coadministered with P-gp and/or BCRP inhibitors. Neither ledipasvir nor sofosbuvir is a substrate for hepatic uptake transporters OCT1, OATP1B1, or OATP1B3. GS-331007 is not a substrate for renal transporters, including organic anion transporter OAT1 or OAT3, or organic cation transporter OCT2.
Ledipasvir is subject to slow oxidative metabolism via an unknown mechanism. In vitro, no detectable metabolism of ledipasvir by CYP enzymes has been observed. Biliary excretion of unchanged ledipasvir is a major route of elimination. Sofosbuvir is not a substrate for CYP and UGT1A1 enzymes. Clinically significant drug interactions with HARVONI mediated by CYP or UGT1A1 enzymes are not expected.
The effects of coadministered drugs on the exposure of ledipasvir, sofosbuvir, and GS-331007 are shown in Table 8 [see Drug Interactions (7)].
Table 8 Drug Interactions: Changes in Pharmacokinetic Parameters for Ledipasvir, Sofosbuvir, and the Predominant Circulating Metabolite GS-331007 in the Presence of the Coadministered Drug All interaction studies conducted in healthy volunteers. Coadministered Drug Dose of Coadministered Drug (mg) Ledipasvir Dose (mg) Sofosbuvir Dose (mg) N Mean Ratio (90% CI) of Ledipasvir, Sofosbuvir, and GS-331007 PK With/Without Coadministered Drug No Effect=1.00 Cmax AUC Cmin NA = not available/not applicable, ND = not dosed. tenofovir DF = tenofovir disoproxil fumarate Atazanavir/ ritonavir + emtricitabine/ tenofovir DF Data generated from simultaneous dosing with HARVONI. Staggered administration (12 hours apart) of atazanavir/ritonavir + emtricitabine/tenofovir DF or darunavir/ritonavir + emtricitabine/tenofovir DF and HARVONI provided similar results. ,The effects of atazanavir/ritonavir on ledipasvir and sofosbuvir are similar with or without the presence of emtricitabine/tenofovir DF. 300/100 + 200/300 once daily 90 once daily 400 once daily 24 ledipasvir 1.68 (1.54, 1.84) 1.96 (1.74, 2.21) 2.18 (1.91, 2.50) sofosbuvir 1.01 (0.88, 1.15) 1.11 (1.02, 1.21) NA GS-331007 1.17 (1.12, 1.23) 1.31 (1.25, 1.36) 1.42 (1.34, 1.49) Carbamazepine 300 twice daily ND 400 single dose 24 sofosbuvir 0.52 (0.43, 0.62) 0.52 (0.46, 0.59) NA GS-331007 1.04 (0.97, 1.11) 0.99 (0.94, 1.04) NA Cyclosporine 600 single dose ND 400 single dose 19 sofosbuvir 2.54 (1.87, 3.45) 4.53 (3.26, 6.30) NA GS-331007 0.60 (0.53, 0.69) 1.04 (0.90, 1.20) NA Darunavir/ ritonavir 800/100 once daily 90 once daily ND 23 ledipasvir 1.45 (1.34, 1.56) 1.39 (1.28, 1.49) 1.39 (1.29, 1.51) ND 400 single dose 18 sofosbuvir 1.45 (1.10, 1.92) 1.34 (1.12, 1.59) NA GS-331007 0.97 (0.90, 1.05) 1.24 (1.18, 1.30) NA Darunavir/ ritonavir + emtricitabine/ tenofovir DF 800/100 + 200/300 once daily 90 once daily 400 once daily 23 ledipasvir 1.11 (0.99, 1.24) 1.12 (1.00, 1.25) 1.17 (1.04, 1.31) sofosbuvir 0.63 (0.52, 0.75) 0.73 (0.65, 0.82) NA GS-331007 1.10 (1.04, 1.16) 1.20 (1.16, 1.24) 1.26 (1.20, 1.32) Efavirenz/ emtricitabine/ tenofovir DF Administered as ATRIPLA¬ģ (efavirenz, emtricitabine, tenofovir DF). 600/200/300 once daily 90 once daily 400 once daily 14 ledipasvir 0.66 (0.59, 0.75) 0.66 (0.59, 0.75) 0.66 (0.57, 0.76) sofosbuvir 1.03 (0.87, 1.23) 0.94 (0.81, 1.10) NA GS-331007 0.86 (0.76, 0.96) 0.90 (0.83, 0.97) 1.07 (1.02, 1.13) Elvitegravir/ cobicistat/ emtricitabine/ tenofovir alafenamide 150/150/200/10 once daily 90 once daily 400 once daily 30 ledipasvir 1.65 (1.53, 1.78) 1.79 (1.64, 1.96) 1.93 (1.74, 2.15) sofosbuvir 1.28 (1.13, 1.47) 1.47 (1.35,1.59) NA GS-331007 1.29 (1.24, 1.35) 1.48 (1.44, 1.53) 1.66 (1.60, 1.73) Famotidine 40 single dose simultaneously with HARVONI 90 single dose 400 single dose 12 ledipasvir 0.80 (0.69, 0.93) 0.89 (0.76, 1.06) NA sofosbuvir 1.15 (0.88, 1.50) 1.11 (1.00, 1.24) NA GS-331007 1.06 (0.97, 1.14) 1.06 (1.02, 1.11) NA 40 single dose 12 hours prior to HARVONI 12 ledipasvir 0.83 (0.69, 1.00) 0.98 (0.80, 1.20) NA sofosbuvir 1.00 (0.76, 1.32) 0.95 (0.82, 1.10) NA GS-331007 1.13 (1.07, 1.20) 1.06 (1.01, 1.12) NA Methadone 30 to 130 daily ND 400 once daily 14 sofosbuvir 0.95 (0.68, 1.33) 1.30 (1.00, 1.69) NA GS-331007 0.73 (0.65, 0.83) 1.04 (0.89, 1.22) NA Omeprazole 20 once daily simultaneously with HARVONI 90 single dose 400 single dose 16 ledipasvir 0.89 (0.61, 1.30) 0.96 (0.66, 1.39) NA sofosbuvir 1.12 (0.88, 1.42) 1.00 (0.80, 1.25) NA GS-331007 1.14 (1.01, 1.29) 1.03 (0.96, 1.12) NA 20 once daily 2 hours prior to ledipasvir 30 single dose ND 17 ledipasvir 0.52 (0.41, 0.66) 0.58 (0.48, 0.71) NA Rifabutin 300 once daily ND 400 single dose 20 sofosbuvir 0.64 (0.53, 0.77) 0.76 (0.63, 0.91) NA GS-331007 1.15 (1.03, 1.27) 1.03 (0.95, 1.12) NA Rifampin 600 once daily 90 single dose This study was conducted in the presence of two other investigational HCV direct-acting agents. ND 31 ledipasvir 0.65 (0.56, 0.76) 0.41 (0.36, 0.48) NA ND 400 single dose 17 sofosbuvir 0.23 (0.19, 0.29) 0.28 (0.24, 0.32) NA GS-331007 1.23 (1.14, 1.34) 0.95 (0.88, 1.03) NA Simeprevir 150 once daily 30 once daily ND 22 ledipasvir 1.81 (1.69, 2.94) 1.92 (1.77, 2.07) NA Tacrolimus 5 single dose ND 400 single dose 16 sofosbuvir 0.97 (0.65, 1.43) 1.13 (0.81, 1.57) NA GS-331007 0.97 (0.83, 1.14) 1.00 (0.87, 1.13) NA
No effect on the pharmacokinetic parameters of ledipasvir, sofosbuvir, and GS-331007 was observed with raltegravir and the combination of abacavir and lamivudine; emtricitabine, rilpivirine, and tenofovir disoproxil fumarate; or dolutegravir, emtricitabine, and tenofovir disoproxil fumarate.
Ledipasvir is an inhibitor of drug transporter P-gp and breast cancer resistance protein (BCRP) and may increase intestinal absorption of coadministered substrates for these transporters. Ledipasvir is an inhibitor of transporters OATP1B1, OATP1B3, and BSEP only at concentrations exceeding those achieved in clinic. Ledipasvir is not an inhibitor of transporters MRP2, MRP4, OCT2, OAT1, OAT3, MATE1, and OCT1. The drug-drug interaction potential of ledipasvir is primarily limited to the intestinal inhibition of P-gp and BCRP. Clinically relevant transporter inhibition by ledipasvir in the systemic circulation is not expected due to its high protein binding. Sofosbuvir and GS-331007 are not inhibitors of drug transporters P-gp, BCRP, MRP2, BSEP, OATP1B1, OATP1B3, and OCT1, and GS-331007 is not an inhibitor of OAT1, OCT2, and MATE1.
Ledipasvir, sofosbuvir, and GS-331007 are not inhibitors or inducers of CYP or UGT1A1 enzymes.
The effects of ledipasvir or sofosbuvir on the exposure of coadministered drugs are shown in Table 9 [see Drug Interactions (7)].
Table 9 Drug Interactions: Changes in Pharmacokinetic Parameters for Coadministered Drug in the Presence of Ledipasvir, Sofosbuvir, or HARVONI All interaction studies conducted in healthy volunteers. Coadministered Drug Dose of Coadministered Drug (mg) Ledipasvir Dose (mg) Sofosbuvir Dose (mg) N Mean Ratio (90% CI) of Coadministered Drug PK With/Without Ledipasvir, Sofosbuvir, or HARVONI No Effect=1.00 Cmax AUC Cmin NA = not available/not applicable, ND = not dosed. tenofovir DF = tenofovir disoproxil fumarate Atazanavir/ ritonavir + emtricitabine /tenofovir DF Data generated from simultaneous dosing with HARVONI. Staggered administration (12 hours apart) of atazanavir/ritonavir + emtricitabine/tenofovir DF or darunavir/ritonavir + emtricitabine/tenofovir DF and HARVONI provided similar results. ,The effects of HARVONI on atazanavir and ritonavir are similar with or without the presence of emtricitabine/tenofovir DF. ,This magnitude of change in tenofovir exposure does not reflect the approximately 60‚Äď80% increase caused by the effects of an HIV PI/ritonavir and the effect of food. Therefore, tenofovir exposure is approximately 130% higher when administered as tenofovir DF + atazanavir/ritonavir + HARVONI or tenofovir DF + darunavir/ritonavir + HARVONI and with food as compared to the tenofovir exposure observed following fasted administration of tenofovir DF-based regimens that do not contain an HIV PI/ritonavir and HARVONI. atazanavir 300 once daily 90 once daily 400 once daily 24 1.07 (0.99, 1.14) 1.27 (1.18, 1.37) 1.63 (1.45, 1.84) ritonavir 100 once daily 0.86 (0.79, 0.93) 0.97 (0.89, 1.05) 1.45 (1.27, 1.64) tenofovir DF 300 once daily 1.47 (1.37, 1.58) 1.35 (1.29, 1.42) 1.47 (1.38, 1.57) Darunavir/ ritonavir + emtricitabine/ tenofovir DF , darunavir 800 once daily 90 once daily 400 once daily 23 1.01 (0.96, 1.06) 1.04 (0.99, 1.08) 1.08 (0.98, 1.20) ritonavir 100 once daily 1.17 (1.01, 1.35) 1.25 (1.15, 1.36) 1.48 (1.34, 1.63) tenofovir DF 300 once daily 1.64 (1.54, 1.74) 1.50 (1.42, 1.59) 1.59 (1.49, 1.70) Elvitegravir/ cobicistat/ emtricitabine/ tenofovir alafenamide elvitegravir 150 once daily 90 once daily 400 once daily 30 0.98 (0.90, 1.07) 1.11 (1.02, 1.20) 1.46 (1.28, 1.66) cobicistat 150 once daily 1.23 (1.15, 1.32) 1.53 (1.45, 1.62) 3.25 (2.88, 3.67) tenofovir alafenamide 10 once daily 0.90 (0.73, 1.11) 0.86 (0.78, 0.95) NA Norelgestromin norgestimate 0.180/0.215/0.25/ethinyl estradiol 0.025 once daily 90 once daily ND 15 1.02 (0.89, 1.16) 1.03 (0.90, 1.18) 1.09 (0.91, 1.31) ND 400 once daily 1.07 (0.94, 1.22) 1.06 (0.92, 1.21) 1.07 (0.89, 1.28) Norgestrel 90 once daily ND 1.03 (0.87, 1.23) 0.99 (0.82, 1.20) 1.00 (0.81, 1.23) ND 400 once daily 1.18 (0.99, 1.41) 1.19 (0.98, 1.45) 1.23 (1.00, 1.51) Ethinyl estradiol 90 once daily ND 1.40 (1.18, 1.66) 1.20 (1.04, 1.39) 0.98 (0.79, 1.22) ND 400 once daily 1.15 (0.97, 1.36) 1.09 (0.94, 1.26) 0.99 (0.80, 1.23) Midazolam 2.5 single dose 90 single dose ND 30 1.07 (1.00, 1.14) 0.99 (0.95, 1.04) NA 0.95 (0.87, 1.04) 0.89 (0.84, 0.95) NA Raltegravir 400 twice daily 90 once daily ND 28 0.82 (0.66, 1.02) 0.85 (0.70, 1.02) 1.15 (0.90, 1.46) ND 400 single dose 19 0.57 (0.44, 0.75) 0.73 (0.59, 0.91) 0.95 (0.81, 1.12) Simeprevir 150 once daily 30 once daily ND 22 2.61 (2.39, 2.86) 2.69 (2.44, 2.96) NA Tacrolimus 5 single dose ND 400 single dose 16 0.73 (0.59, 0.90) 1.09 (0.84, 1.40) NA Tenofovir DF 300 once daily Administered as ATRIPLA (efavirenz, emtricitabine, tenofovir DF). The effects of HARVONI on tenofovir exposures are similar when tenofovir is administered as ATRIPLA, COMPLERA, or TRUVADA + dolutegravir. 90 once daily 400 once daily 15 1.79 (1.56, 2.04) 1.98 (1.77, 2.23) 2.63 (2.32, 2.97)
No effect on the pharmacokinetic parameters of the following coadministered drugs was observed with ledipasvir or sofosbuvir: abacavir, cyclosporine, darunavir/ritonavir, dolutegravir, efavirenz, emtricitabine, lamivudine, methadone, or rilpivirine.
12.4 Microbiology
Mechanism of Action
Ledipasvir is an inhibitor of the HCV NS5A protein, which is required for viral replication. Resistance selection in cell culture and cross-resistance studies indicate ledipasvir targets NS5A as its mode of action.
Sofosbuvir is an inhibitor of the HCV NS5B RNA-dependent RNA polymerase, which is required for viral replication. Sofosbuvir is a nucleotide prodrug that undergoes intracellular metabolism to form the pharmacologically active uridine analog triphosphate (GS-461203), which can be incorporated into HCV RNA by the NS5B polymerase and acts as a chain terminator. In a biochemical assay, GS-461203 inhibited the polymerase activity of the recombinant NS5B from HCV genotypes 1b and 4a with IC50 values of 3.3 and 2.7 microM, respectively. GS-461203 is neither an inhibitor of human DNA and RNA polymerases nor an inhibitor of mitochondrial RNA polymerase.
Antiviral Activity
In HCV replicon assays, the EC50 values of ledipasvir against full-length replicons from genotypes 1a and 1b were 0.031 nM and 0.004 nM, respectively. The median EC50 values of ledipasvir against chimeric replicons encoding NS5A sequences from clinical isolates from treatment-na√Įve HCV-infected subjects were 0. 02 nM for genotype 1a (range 0.007‚Äď1.0 nM; N=23) and 0.006 nM for genotype 1b (range 0.002‚Äď1.0 nM; N=34). Ledipasvir had median EC50 values ranging between 0.002 nM to 0.16 nM against 11 genotype 4 subtypes (4a, 4d, 4n, 4r, 4o, 4c, 4f, 4k, 4l, 4m, and 4t). The median EC50 value for subtype 4b was 199.6 nM (range 0.66‚Äď1799 nM; N=3); the two 4b isolates with EC50 values greater than 100 nM had NS5A resistance-associated polymorphisms L30S+M31M+P58S+Y93H. The median EC50 value of ledipasvir was 0.03 nM against genotype 5a isolates (range 0.008‚Äď0.081 nM; N=35). For genotype 6, the EC50 values for ledipasvir varied by subtype. Subtypes 6a and 6h had median EC50 values of 0.55 and 0.17 nM, respectively. For subtypes 6e, 6l, 6n, 6q, 6k, and 6m, the median EC50 values ranged from 60.6 nM to 430.1 nM.
In HCV replicon assays, the EC50 values of sofosbuvir against full-length replicons from genotypes 1a, 1b, and 4a, and chimeric 1b replicons encoding NS5B from genotypes 5a or 6a ranged from 14‚Äď110 nM. The median EC50 value of sofosbuvir against chimeric replicons encoding NS5B sequences from clinical isolates was 62 nM for genotype 1a (range 29‚Äď128 nM; N=67) and 102 nM for genotype 1b (range 45‚Äď170 nM; N=29). In replication competent virus assays, the EC50 value of sofosbuvir against genotype 1a was 30 nM. Evaluation of sofosbuvir in combination with ledipasvir showed no antagonistic effect in reducing HCV RNA levels in replicon cells.
Resistance
In Cell Culture
HCV replicons with reduced susceptibility to ledipasvir have been selected in cell culture for genotypes 1a and 1b. Reduced susceptibility to ledipasvir was associated with the primary NS5A amino acid substitution Y93H in both genotypes 1a and 1b. Additionally, a Q30E substitution emerged in genotype 1a replicons. Site-directed mutagenesis of the Y93H in both genotypes 1a and 1b, as well as the Q30E substitution in genotype 1a, conferred high levels of reduced susceptibility to ledipasvir (fold change in EC50 greater than 1000-fold).
HCV replicons with reduced susceptibility to sofosbuvir have been selected in cell culture for multiple genotypes including 1b, 4a, 5a, and 6a. Reduced susceptibility to sofosbuvir was associated with the NS5B substitution S282T in all replicon genotypes examined. An M289L substitution developed along with the S282T substitution in genotype 5 and 6 replicons. Site-directed mutagenesis of the S282T substitution in replicons of 8 genotypes conferred 2- to 18-fold reduced susceptibility to sofosbuvir.
In Clinical Trials
Persistence of Resistance-Associated Substitutions
No data are available on the persistence of ledipasvir or sofosbuvir resistance-associated substitutions. NS5A resistance-associated substitutions for other NS5A inhibitors have been found to persist for >1 year in some patients. The long-term clinical impact of the emergence or persistence of virus containing ledipasvir or sofosbuvir resistance-associated substitutions is unknown.
Effect of Baseline HCV Polymorphisms on Treatment Response
Adults
Pediatrics
In Study 1116, the presence of NS5A and NS5B resistance-associated polymorphisms did not impact treatment outcome; all pediatric subjects 3 years of age and older with baseline NS5A or NS5B nucleoside inhibitor resistance-associated polymorphisms (14%; 32/223) achieved SVR following 12 weeks treatment with HARVONI.
Cross Resistance
Based on resistance patterns observed in cell culture replicon studies and HCV-infected subjects, cross-resistance between ledipasvir and other NS5A inhibitors is expected. Both sofosbuvir and ledipasvir were fully active against substitutions associated with resistance to other classes of direct-acting antivirals with different mechanisms of action, such as NS5B non-nucleoside inhibitors and NS3 protease inhibitors. The efficacy of ledipasvir/sofosbuvir has not been established in patients who have previously failed treatment with other regimens that include an NS5A inhibitor.
13 Nonclinical Toxicology
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Carcinogenesis and Mutagenesis
Ledipasvir: Ledipasvir was not genotoxic in a battery of in vitro or in vivo assays, including bacterial mutagenicity, chromosome aberration using human peripheral blood lymphocytes, and in vivo rat micronucleus assays.
Ledipasvir was not carcinogenic in a 6-month rasH2 transgenic mouse study (up to 300 mg/kg/day). Similarly, ledipasvir was not carcinogenic in a 2-year rat study (up to 100 mg/kg/day in males and 30 mg/kg/day in females), resulting in exposures approximately 10 and 4 times, respectively, higher than the exposure in humans at the recommended human dose (RHD).
Sofosbuvir: Sofosbuvir was not genotoxic in a battery of in vitro or in vivo assays, including bacterial mutagenicity, chromosome aberration using human peripheral blood lymphocytes, and in vivo mouse micronucleus assays.
Sofosbuvir was not carcinogenic in a 2-year mouse study (up to 200 mg/kg/day in males and 600 mg/kg/day in females) and in a 2-year rat study (up to 750 mg/kg/day), resulting in exposures of the predominant circulating metabolite GS-331007 of approximately 4 and 18 times (in mice) and 8 and 10 times (in rats), in males and females respectively, the exposure in humans at the RHD.
Impairment of Fertility
Ledipasvir: Ledipasvir had no adverse effects on mating and fertility. In female rats, the mean number of corpora lutea and implantation sites were reduced slightly at maternal exposures approximately 3 times the exposure in humans at the RHD. At the highest dose levels without effects, exposures of ledipasvir were approximately 5 and 2 times, in males and females, respectively, the exposure in humans at the RHD.
Sofosbuvir: Sofosbuvir had no effects on embryo-fetal viability or on fertility when evaluated in rats. At the highest dose tested, exposure to the predominant circulating metabolite GS-331007 was approximately 5 times the exposure in humans at the RHD.
14 Clinical Studies
14.1Description of Clinical Trials
The efficacy and safety of HARVONI were evaluated in four trials in genotype 1 HCV mono-infected subjects including one trial exclusively in treatment-experienced subjects with compensated cirrhosis (Child-Pugh A); one trial in genotype 1 or 4 HCV/HIV-1 coinfected subjects; two trials in genotype 4, 5, or 6 HCV mono-infected subjects; two trials in genotype 1 or 4 HCV infected pretransplant subjects with decompensated cirrhosis (Child-Pugh B and C) or post-transplant with Metavir F0‚ÄďF3 fibrosis, compensated cirrhosis, decompensated cirrhosis, or fibrosing cholestatic hepatitis (FCH); two trials in subjects with severe renal impairment (one of which included subjects requiring dialysis); and one trial in genotype 1 or 4 HCV pediatric subjects 3 years of age and older without cirrhosis or with compensated cirrhosis, as summarized in Table 10 [see Clinical Studies (14.2, 14.3, 14.4, 14.5, 14.6, and 14.7)]:
Table 10 Trials Conducted with HARVONI with or without Ribavirin in Subjects with Chronic HCV Genotype 1, 4, 5, or 6 Infection Trial Population Study Arms (Number of Subjects Treated) ESRD = End stage renal disease; RBV = ribavirin; RI = Renal impairment; TN = Treatment-na√Įve subjects. ION-3 Open-label. (NCT01851330)GT1, TN without cirrhosis HARVONI 8 weeks (215) HARVONI + RBV 8 weeks (216) HARVONI 12 weeks (216) ION-1 (NCT01701401) GT1, TN with or without cirrhosis HARVONI 12 weeks (214) HARVONI + RBV 12 weeks (217) HARVONI 24 weeks (217) HARVONI + RBV 24 weeks (217) ION-2 (NCT01768286) GT1, TE TE = Treatment-experienced subjects including those who have failed a peginterferon alfa + RBV based regimen with or without an HCV protease inhibitor. with or without cirrhosisHARVONI 12 weeks (109) HARVONI + RBV 12 weeks (111) HARVONI 24 weeks (109) HARVONI + RBV 24 weeks (111) SIRIUS Double-blind, placebo-controlled. (NCT01965535)GT1, TE with cirrhosis HARVONI + RBV 12 Weeks (77) HARVONI 24 weeks (77) ION-4 (NCT02073656) GT1 and GT4 HCV/HIV-1 coinfected TN and TE with or without cirrhosis HARVONI 12 Weeks (N=327 for GT1; N=8 for GT4) 1119 (NCT02081079) GT4 and GT5, TN and TE with or without cirrhosis HARVONI 12 Weeks (N=44 for GT4; N=41 for GT5) ELECTRON-2 (NCT01826981) GT6, TN and TE with or without cirrhosis HARVONI 12 Weeks (25) SOLAR-1 and SOLAR-2 (NCT01938430 and NCT02010255) GT1 and GT4 pre-transplant with decompensated cirrhosis or post-transplant with Metavir F0‚ÄďF3 fibrosis, compensated cirrhosis, decompensated cirrhosis, or FCH HARVONI + RBV 12 Weeks (336) HARVONI + RBV 24 weeks (334) 1116 (NCT02249182) GT1 or 4 TN and TE with or without cirrhosis in pediatric subjects 3 years of age and older HARVONI 12 Weeks (223) HARVONI 24 Weeks (1) 0154 (NCT01958281) GT1 TN and TE with severe RI without dialysis HARVONI 12 weeks (18) 4063 (NCT03036839) GT1, 5, or 6 TN and TE TE = Treatment experienced subjects including those who have failed either interferon/peginterferon alfa/ribavirin based regimens or HCV-specific direct-acting antiviral regimens that do not include an NS5A polymerase inhibitor. with or without compensated cirrhosis, with ESRD requiring dialysisHARVONI 8 Weeks (45) HARVONI 12 Weeks (12) HARVONI 24 Weeks (6)
HARVONI was administered once daily by mouth in these trials. For subjects without cirrhosis or with compensated cirrhosis who received ribavirin, the ribavirin dosage was 1000 mg per day for subjects weighing less than 75 kg or 1200 mg per day for subjects weighing at least 75 kg. For subjects with decompensated cirrhosis in SOLAR-1 and SOLAR-2 studies, the starting ribavirin dosage was 600 mg per day regardless of transplantation status. Ribavirin dose adjustments were performed according to the ribavirin labeling.
Serum HCV RNA values were measured during the clinical trials using the COBAS TaqMan HCV test (version 2.0), for use with the High Pure System in ION-3, ION-1, ION-2, SIRIUS, and ION-4 studies or the COBAS AmpliPrep/COBAS Taqman HCV test (version 2.0) in ELECTRON-2, 1119, SOLAR-1, SOLAR-2, and 1116 studies. The COBAS TaqMan HCV test (version 2.0) for use with the High Pure System has a lower limit of quantification (LLOQ) of 25 IU per mL and the COBAS AmpliPrep/COBAS Taqman HCV test (version 2.0) has a LLOQ of 15 IU per mL. Sustained virologic response (SVR12), defined as HCV RNA less than LLOQ at 12 weeks after the cessation of treatment, was the primary endpoint in studies in adults and the key efficacy endpoint in the study in pediatric subjects 12 years of age and older. Relapse was a secondary endpoint, which was defined as HCV RNA greater than or equal to LLOQ with 2 consecutive values or last available post-treatment measurement during the post-treatment period after achieving HCV RNA less than LLOQ at end of treatment.
14.2Clinical Trials in Subjects with Genotype 1 HCV
Treatment-Na√Įve Adults without Cirrhosis ‚Äď ION-3 (Study 0108)
ION-3 was a randomized, open-label trial in treatment-na√Įve non-cirrhotic subjects with genotype 1 HCV. Subjects were randomized in a 1:1:1 ratio to one of the following three treatment groups and stratified by HCV genotype (1a vs 1b): HARVONI for 8 weeks, HARVONI for 12 weeks, or HARVONI + ribavirin for 8 weeks.
Demographics and baseline characteristics were balanced across the treatment groups. Of the 647 treated subjects, the median age was 55 years (range: 20 to 75); 58% of the subjects were male; 78% were White; 19% were Black; 6% were Hispanic or Latino; mean body mass index was 28 kg/m2 (range: 18 to 56 kg/m2); 81% had baseline HCV RNA levels greater than or equal to 800,000 IU per mL; 80% had genotype 1a HCV infection; 73% had non-C/C IL28B alleles (CT or TT).
Table 11 presents the SVR12 for the HARVONI treatment groups in the ION-3 trial after 8 and 12 weeks of HARVONI treatment. Ribavirin was not shown to increase the SVR12 observed with HARVONI. Therefore, the HARVONI + ribavirin arm is not presented in Table 11.
Table 11 Study ION-3: SVR12 after 8 and 12 Weeks of Treatment in Treatment-Na√Įve Non-Cirrhotic Subjects with Genotype 1 HCV HARVONI 8 Weeks (N=215) HARVONI 12 Weeks (N=216) SVR12 94% (202/215) 96% (208/216) Outcome for Subjects without SVR ¬†¬†On-Treatment Virologic Failure 0/215 0/216 ¬†¬†Relapse The denominator for relapse is the number of subjects with HCV RNA <LLOQ at their last on-treatment assessment. 5% (11/215) 1% (3/216) ¬†¬†Other Other includes subjects who did not achieve SVR and did not meet virologic failure criteria (e.g., lost to follow-up). 1% (2/215) 2% (5/216) SVR by Genotype One subject without a confirmed subtype for genotype 1 infection was excluded from this subgroup analysis. ¬†¬†Genotype 1a 93% (159/171) 96% (165/172) ¬†¬†Genotype 1b 98% (42/43) 98% (43/44)
The treatment difference between the 8-week treatment of HARVONI and 12-week treatment of HARVONI was ‚ąí2.3% (97.5% confidence interval ‚ąí7.2% to 2.5%). Among subjects with a baseline HCV RNA less than 6 million IU per mL, the SVR12 was 97% (119/123) with 8-week treatment of HARVONI and 96% (126/131) with 12-week treatment of HARVONI.
Relapse rates by baseline viral load are presented in Table 12.
Table 12 Study ION-3: Relapse Rates by Baseline Viral Load after 8 and 12 Weeks of Treatment in Treatment-Na√Įve Non-Cirrhotic Subjects with Genotype 1 HCV HARVONI 8 Weeks (N=215) HARVONI 12 Weeks (N=216) Number of Responders at End of Treatment 215 216 Baseline HCV RNA HCV RNA values were determined using the Roche TaqMan Assay; a subject's HCV RNA may vary from visit to visit. ¬†¬†HCV RNA <6 million IU/mL 2% (2/123) 2% (2/131) ¬†¬†HCV RNA ‚Č•6 million IU/mL 10% (9/92) 1% (1/85)
Treatment-Na√Įve Adults with or without Cirrhosis ‚Äď ION-1 (Study 0102)
ION-1 was a randomized, open-label trial that evaluated 12 and 24 weeks of treatment with HARVONI with or without ribavirin in 865 treatment-na√Įve subjects with genotype 1 HCV including those with cirrhosis. Subjects were randomized in a 1:1:1:1 ratio to receive HARVONI for 12 weeks, HARVONI + ribavirin for 12 weeks, HARVONI for 24 weeks, or HARVONI + ribavirin for 24 weeks. Randomization was stratified by the presence or absence of cirrhosis and HCV genotype (1a vs 1b).
Demographics and baseline characteristics were balanced across the treatment groups. Of the 865 treated subjects, the median age was 54 years (range: 18 to 80); 59% of the subjects were male; 85% were White; 12% were Black; 12% were Hispanic or Latino; mean body mass index was 27 kg/m2 (range: 18 to 48 kg/m2); 79% had baseline HCV RNA levels greater than or equal to 800,000 IU per mL; 67% had genotype 1a HCV infection; 70% had non-C/C IL28B alleles (CT or TT); and 16% had cirrhosis.
Table 13 presents the SVR12 for the treatment group of HARVONI for 12 weeks in the ION-1 trial. Ribavirin was not shown to increase SVR12 observed with HARVONI. Therefore, the HARVONI + ribavirin arm is not presented in Table 13.
Table 13 Study ION-1: SVR12 after 12 Weeks of Treatment in Treatment-Na√Įve Subjects with Genotype 1 HCV with and without Cirrhosis HARVONI 12 Weeks (N=214) SVR12 Excluding one subject with genotype 4 infection. 99% (210/213) Outcome for Subjects without SVR ¬†¬†On-Treatment Virologic Failure 0/213 ¬†¬†Relapse , The denominator for relapse is the number of subjects with HCV RNA <LLOQ at their last on-treatment assessment. <1% (1/212) ¬†¬†Other , Other includes subjects who did not achieve SVR12 and did not meet virologic failure criteria (e.g., lost to follow-up). 1% (2/213)
SVR12 for selected subgroups are presented in Table 14.
Table 14 Study ION-1: SVR12 for Selected Subgroups after 12 Weeks of Treatment in Treatment-Na√Įve Subjects with Genotype 1 HCV with and without Cirrhosis HARVONI 12 Weeks (N=214) Genotype One subject without a confirmed subtype for genotype 1 infection and one subject with genotype 4 infection were excluded from this subgroup analysis. ¬†¬†Genotype 1a 98% (142/145) ¬†¬†Genotype 1b 100% (67/67) Cirrhosis Subjects with missing cirrhosis status were excluded from this subgroup analysis. ¬†¬†No 99% (176/177) ¬†¬†Yes 94% (32/34)
Previously-Treated Adults with or without Cirrhosis ‚Äď ION-2 (Study 0109)
ION-2 was a randomized, open-label trial that evaluated 12 and 24 weeks of treatment with HARVONI with or without ribavirin in genotype 1 HCV-infected subjects with or without cirrhosis who failed prior therapy with an interferon-based regimen, including regimens containing an HCV protease inhibitor. Subjects were randomized in a 1:1:1:1 ratio to receive HARVONI for 12 weeks, HARVONI + ribavirin for 12 weeks, HARVONI for 24 weeks, or HARVONI + ribavirin for 24 weeks. Randomization was stratified by the presence or absence of cirrhosis, HCV genotype (1a vs 1b) and response to prior HCV therapy (relapse/breakthrough vs nonresponse).
Demographics and baseline characteristics were balanced across the treatment groups. Of the 440 treated subjects, the median age was 57 years (range: 24 to 75); 65% of the subjects were male; 81% were White; 18% were Black; 9% were Hispanic or Latino; mean body mass index was 28 kg/m2 (range: 19 to 50 kg/m2); 89% had baseline HCV RNA levels greater than or equal to 800,000 IU per mL; 79% had genotype 1a HCV infection; 88% had non-C/C IL28B alleles (CT or TT); and 20% had cirrhosis. Forty-seven percent (47%) of the subjects failed a prior therapy of pegylated interferon and ribavirin. Among these subjects, 49% were relapse/breakthrough and 51% were non-responder. Fifty-three percent (53%) of the subjects failed a prior therapy of pegylated interferon and ribavirin with an HCV protease inhibitor. Among these subjects, 62% were relapse/breakthrough and 38% were non-responder.
Table 15 presents the SVR12 for the HARVONI treatment groups in the ION-2 trial. Ribavirin was not shown to increase SVR12 observed with HARVONI. Therefore, the HARVONI + ribavirin arms are not presented in Table 15.
Table 15 Study ION-2: SVR12 after 12 and 24 Weeks of Treatment in Subjects with Genotype 1 HCV with or without Cirrhosis Who Failed Prior Therapy HARVONI 12 Weeks (N=109) HARVONI 24 Weeks (N=109) SVR12 94% (102/109) 99% (108/109) Outcome for Subjects without SVR   On-Treatment Virologic Failure 0/109 0/109   Relapse The denominator for relapse is the number of subjects with HCV RNA <LLOQ at their last on-treatment assessment. 6% (7/108) 0/109   Other Other includes subjects who did not achieve SVR12 and did not meet virologic failure criteria (e.g., lost to follow-up). 0/109 1% (1/109)
Among the subjects with available SVR12 and SVR24 data (206/218), all subjects who achieved SVR12 in the ION-2 study also achieved SVR24.
SVR12 and relapse rates for selected subgroups are presented in Tables 16 and 17.
Table 16 Study ION-2: SVR12 for Selected Subgroups after 12 and 24 Weeks of Treatment in Subjects with Genotype 1 HCV Who Failed Prior Therapy HARVONI 12 Weeks (N=109) HARVONI 24 Weeks (N=109) RBV = ribavirin. Genotype   Genotype 1a 95% (82/86) 99% (84/85)   Genotype 1b 87% (20/23) 100% (24/24) Cirrhosis Subjects with missing cirrhosis status were excluded from this subgroup analysis.   No 95% (83/87) 99% (85/86)   Yes 86% (19/22) 100% (22/22) Prior HCV Therapy   Peg-IFN + RBV 93% (40/43) 100% (58/58)   HCV protease inhibitor + Peg-IFN + RBV 94% (62/66) 98% (49/50) Response to Prior HCV Therapy   Relapse/Breakthrough 95% (57/60) 100% (60/60)   Non-responder 92% (45/49) 98% (48/49)
Table 17 Study ION-2: Relapse Rates for Selected Subgroups after 12 and 24 Weeks of Treatment in Subjects with Genotype 1 HCV Who Failed Prior Therapy HARVONI 12 Weeks (N=109) HARVONI 24 Weeks (N=109) Number of Responders at End of Treatment 108 109 Cirrhosis Subjects with missing cirrhosis status were excluded from this subgroup analysis.   No 5% (4/86) These 4 non-cirrhotic relapsers all had baseline NS5A resistance-associated polymorphisms. 0% (0/86)   Yes 14% (3/22) 0% (0/22) Presence of Baseline NS5A Resistance-Associated Polymorphisms NS5A resistance-associated polymorphisms include any change at NS5A positions 24, 28, 30, 31, 58, 92, or 93.   No 2% (2/85) 0% (0/90)   Yes 22% (5/23) 0% (0/19) IL28B Status   C/C 0% (0/10) 0% (0/16)   Non-C/C 7% (7/98) 0% (0/93)
Previously-Treated Adults with Cirrhosis ‚Äď SIRIUS (Study 0121)
SIRIUS was a randomized, double-blind and placebo-controlled trial that evaluated the efficacy of HARVONI + ribavirin for 12 weeks or HARVONI without ribavirin for 24 weeks in genotype 1 HCV-infected subjects with compensated cirrhosis who failed prior therapy with a Peg-IFN + ribavirin regimen followed by a subsequent Peg-IFN + ribavirin + an HCV protease inhibitor regimen. Subjects were randomized in a 1:1 ratio to receive placebo for 12 weeks followed by HARVONI + ribavirin for 12 weeks or HARVONI for 24 weeks. Randomization was stratified by HCV genotype (1a vs 1b) and response to prior HCV therapy (never achieved HCV RNA less than LLOQ vs achieved HCV RNA less than LLOQ).
Demographics and baseline characteristics were balanced across the treatment groups. Of the 155 randomized subjects, the median age was 56 years (range: 23 to 77); 74% of the subjects were male; 97% were White; mean body mass index was 27 kg/m2 (range: 19 to 47 kg/m2); 63% had genotype 1a HCV infection; 94% had non-C/C IL28B alleles (CT or TT). One subject discontinued therapy while on placebo, and was not included in the efficacy analysis.
The SVR12 was 96% (74/77) and 97% (75/77) in subjects treated with HARVONI + ribavirin for 12 weeks and HARVONI for 24 weeks without ribavirin, respectively. All 5 subjects who did not achieve SVR12 relapsed.
14.3Clinical Trials in Subjects with Genotype 4, 5, or 6 HCV
Below are trial descriptions, SVR12, and relapse data in the genotype 4, 5, and 6 HCV populations. Trial results in the genotype 4, 5, and 6 HCV populations are based upon limited number of subjects in some subgroups, particularly in subjects who have been previously treated and subjects with cirrhosis.
Genotype 4
In two open-label studies (Study 1119 and ION-4), HARVONI was administered for 12 weeks to treatment-na√Įve and previously-treated adult subjects with genotype 4 HCV infection. Study 1119 enrolled 44 treatment-na√Įve or previously-treated subjects with genotype 4 HCV, with or without cirrhosis. ION-4 enrolled 4 treatment-na√Įve and 4 previously-treated subjects with genotype 4 HCV infection who were coinfected with HIV-1, none of whom had cirrhosis.
In Study 1119, the overall SVR12 rate was 93% (41/44). SVR12 was similar based upon prior HCV treatment history and cirrhosis status. In ION-4, all 8 subjects achieved SVR12.
Genotype 5
In the open-label 1119 trial, HARVONI was administered for 12 weeks to 41 treatment-na√Įve or previously treated adult subjects with genotype 5 HCV infection, with or without cirrhosis. The overall SVR12 was 93% (38/41). SVR12 was similar based upon prior HCV treatment history and cirrhosis status.
Genotype 6
In the open-label ELECTRON-2 trial, HARVONI was administered for 12 weeks to 25 treatment-na√Įve or previously treated adult subjects with genotype 6 HCV infection, with or without cirrhosis. The overall SVR12 was 96% (24/25). SVR12 was similar based upon prior HCV treatment history and cirrhosis status. The single subject who relapsed discontinued study treatment early (at approximately Week 8).
14.4Clinical Trials in Subjects Coinfected with HCV and HIV-1
ION-4 was an open-label clinical trial that evaluated the safety and efficacy of 12 weeks of treatment with HARVONI without ribavirin in HCV treatment-na√Įve and previously treated adult subjects with genotype 1 or 4 HCV infection who were coinfected with HIV-1. Treatment-experienced subjects had failed prior treatment with Peg-IFN + ribavirin, Peg-IFN + ribavirin + an HCV protease inhibitor, or sofosbuvir + ribavirin. Subjects were on a stable HIV-1 antiretroviral therapy that included emtricitabine + tenofovir disoproxil fumarate, administered with efavirenz, rilpivirine, or raltegravir.
Of the 335 treated subjects, the median age was 52 years (range: 26 to 72); 82% of the subjects were male; 61% were White; 34% were Black; mean body mass index was 27 kg/m2 (range: 18 to 66 kg/m2); 75% had genotype 1a HCV infection; 2% had genotype 4 infection; 76% had non-C/C IL28B alleles (CT or TT); and 20% had compensated cirrhosis. Fifty-five percent (55%) of the subjects were treatment-experienced.
Table 18 presents the SVR12 in the ION-4 trial after 12 weeks of HARVONI treatment.
Table 18 Study ION-4: SVR12 in Subjects with Genotype 1 or 4 HCV Coinfected with HIV-1 HARVONI 12 Weeks (N=335) SVR12 96% (321/335) Outcome for Subjects without SVR   On-Treatment Virologic Failure <1% (2/335)   Relapse The denominator for relapse is the number of subjects with HCV RNA <LLOQ at their last on-treatment assessment. 3% (10/333)   Other Other includes subjects who did not achieve SVR12 and did not meet virologic failure criteria (e.g., lost to follow-up). <1% (2/335)
SVR12 rates were 94% (63/67) in subjects with cirrhosis and 98% (46/47) in subjects who were previously treated and had cirrhosis. The relapse rate in the ION-4 trial in Black subjects was 9% (10/115), all of whom were IL28B non-CC genotype, and none in non-Black subjects (0/220). In the ION-1, ION-2, and ION-3 HCV mono-infection studies, relapse rates were 3% (10/305) in Black subjects and 2% (26/1637) in non-Black subjects.
No subject had HIV-1 rebound during the study. The percentage of CD4+ cells did not change during treatment. Median CD4+ cell count increase of 29 cells/mm3 was observed at the end of treatment with HARVONI for 12 weeks.
14.5Clinical Trials in Liver Transplant Recipients and/or Subjects with Decompensated Cirrhosis
SOLAR-1 and SOLAR-2 were two open-label trials that evaluated 12 and 24 weeks of treatment with HARVONI in combination with ribavirin in HCV treatment-na√Įve and previously treated adult subjects with genotype 1 and 4 infection who had undergone liver transplantation and/or who had decompensated liver disease. The two trials were identical in study design. Subjects were enrolled in one of the seven groups in the trials based on liver transplantation status and severity of hepatic impairment (see Table 19). Subjects with a CPT score greater than 12 were excluded. Within each group, subjects were randomized in a 1:1 ratio to receive HARVONI + ribavirin for 12 weeks or HARVONI + ribavirin for 24 weeks. For subjects with decompensated cirrhosis in SOLAR-1 and SOLAR-2 studies, the starting ribavirin dosage was 600 mg per day regardless of transplantation status. Ribavirin dose adjustments were performed according to the ribavirin labeling [see Clinical Studies (14.1)].
Demographics and baseline characteristics were balanced across the treatment groups. Of the 670 treated subjects, the median age was 59 years (range: 21 to 81); 77% of the subjects were male; 91% were White; mean body mass index was 28 kg/m2 (range: 18 to 49 kg/m2); 94% and 6% had genotype 1 and 4 HCV infection, respectively; 78% of the subjects failed a prior HCV therapy.
Table 19 presents the pooled SVR12 rates for SOLAR-1 and SOLAR-2 in subjects with genotype 1 HCV treated with HARVONI + ribavirin for 12 weeks. The SVR12 rates observed with 24 weeks of HARVONI + ribavirin were similar to the SVR12 rates observed with 12 weeks of treatment. Therefore, the results for the HARVONI + ribavirin 24 weeks arm are not presented in Table 19.
Table 19 Studies SOLAR-1 and SOLAR-2: SVR12 and Relapse Rates After 12 Weeks of Treatment with HARVONI and Ribavirin in Subjects with Genotype 1 HCV Who Were Post Liver Transplant and/or Who Had Decompensated Liver Disease HARVONI + RBV 12 weeks (N=307) SVR12 (N=300) Five subjects transplanted prior to post-treatment Week 12 with HCV RNA<LLOQ at last measurement prior to transplant were excluded. ,Two subjects were excluded due to failure to meet the inclusion criteria for any of the treatment groups (i.e., did not have decompensated cirrhosis and had also not received a liver transplant). Relapse (N=288) , , Twelve subjects were excluded from relapse analysis because they died (N=11) or withdrew consent (N=1) prior to reaching the 12-week post-treatment follow-up visit. Pre-transplant ¬†¬†CPT B 87% (45/52) 12% (6/51) ¬†¬†CPT C 88% (35/40) 5% (2/37) Post-transplant ¬†¬†Metavir score F0‚ÄďF3 95% (94/99) 3% (3/97) ¬†¬†CPT A 98% (55/56) 0% (0/55) ¬†¬†CPT B 89% (41/46) 2% (1/42) ¬†¬†CPT C 57% (4/7) 33% (2/6)
There were 7 subjects with fibrosing cholestatic hepatitis in the 12-week treatment arm, and all subjects achieved SVR12.
In genotype 4 HCV post-transplant subjects without cirrhosis or with compensated cirrhosis treated with HARVONI + ribavirin for 12 weeks (N=12), the SVR12 rate was similar to rates reported with genotype 1; no subjects relapsed. Available data in subjects with genotype 4 HCV who had decompensated cirrhosis (pre- and post-liver transplantation) were insufficient for dosing recommendations; therefore, these results are not presented.
14.6 Clinical Trials in Adults with Severe Renal Impairment, Including those Requiring Dialysis
Trial 0154 was an open-label clinical trial that evaluated 12 weeks of treatment with HARVONI in 18 treatment-na√Įve and treatment-experienced (subjects with prior exposure to an HCV NS5B polymerase inhibitor were excluded) genotype 1 HCV-infected adults with severe renal impairment not requiring dialysis. At baseline, two subjects (11%) had cirrhosis and the mean eGFR was 24.9 mL/min (range: 9.0 to 39.6). The SVR rate was 100% (18/18).
As shown in the table below, Trial 4063 was an open-label three-arm clinical trial that evaluated 8, 12, and 24 weeks of treatment with HARVONI in a total of 63 adults with chronic HCV infection and ESRD requiring dialysis. Of the 63 subjects, 10% had cirrhosis, 24% were treatment-experienced, 95% were on hemodialysis, and 5% were on peritoneal dialysis; mean duration on dialysis was 12 years (range: 0.2 to 43 years). The SVR rates for the 8, 12, and 24 week HARVONI treatment groups are shown in Table 20.
Table 20 Trial 4063: SVR12 after 8, 12, and 24 Weeks of Treatment in Adults with HCV with or without Cirrhosis and with Severe Renal Impairment Requiring Dialysis HARVONI 8 Weeks (N=45) HARVONI 12 Weeks (N=12) HARVONI 24 Weeks (N=6) Population Treatment-na√Įve, GT 1 HCV Non-cirrhotic Treatment-na√Įve and treatment- experienced Subjects with prior exposure to any HCV NS5A inhibitor were excluded. GT 1, 5, 6One subject had an indeterminant HCV GT. HCV Non-cirrhoticTreatment-experienced, GT 1 HCV with compensated cirrhosis SVR12 93% (42/45) 100% (12/12) 83% (5/6) Outcome for Subjects without SVR ¬†¬†On-Treatment Virologic Failure 0/45 0/12 0/6 ¬†¬†Relapse 0/44 0/12 0/6 ¬†¬†Other "Other" outcomes includes subjects who did not achieve SVR and did not meet virologic failure criteria. All subjects who failed without virologic relapse or on-treatment virologic failure died prior to follow-up Week 12. None of these deaths were assessed as treatment-related. 7% (3/45) 0/12 17% (1/6) 14.7Clinical Trial in Pediatric Subjects
The efficacy of HARVONI was evaluated in an open-label trial (Study 1116) in 224 HCV treatment-na√Įve (N=186) and treatment-experienced (N=38) pediatric subjects 3 years of age or older. This study evaluated 12 weeks of treatment with HARVONI once daily in genotype 1 (N=183) or genotype 4 (N=3) treatment-naive subjects without cirrhosis or with compensated cirrhosis; genotype 1 treatment-experienced subjects without cirrhosis (N=37); and evaluated 24 weeks of treatment with HARVONI once daily in one genotype 1 subject who was both treatment-experienced and cirrhotic.
Subjects 12 Years to <18 Years of Age: HARVONI was evaluated in 100 subjects 12 years to <18 years of age with HCV genotype 1 infection. Demographics and baseline characteristics were balanced across treatment-na√Įve and treatment-experienced subjects (patients had failed an interferon based regimen with or without ribavirin). The median age was 15 years (range: 12 to 17); 63% of the subjects were female; 91% were White, 7% were Black, and 2% were Asian; 13% were Hispanic/Latino; mean body mass index was 23 kg/m2 (range: 13.1 to 36.6 kg/m2); mean weight was 61 kg (range 33 to 126 kg); 55% had baseline HCV RNA levels greater than or equal to 800,000 IU/mL; 81% had genotype 1a HCV infection. One subject (treatment-na√Įve) had known compensated cirrhosis. The majority of subjects (84%) had been infected through vertical transmission.
The SVR12 rate was 98% overall (98% [78/80] in treatment-na√Įve subjects and 100% [20/20] in treatment-experienced subjects). No subject experienced on-treatment virologic failure or relapse. Two subjects were lost to follow-up.
Subjects 6 Years to <12 Years of Age: HARVONI was evaluated in 90 subjects 6 years to <12 years of age with HCV genotype 1 or 4 infection. Among these subjects, 72 (80%) were treatment-na√Įve and 18 (20%) were treatment-experienced. Eighty-nine of the subjects (87 with genotype 1 HCV infection and 2 with genotype 4 HCV infection) were treated with HARVONI for 12 weeks, 1 subject with genotype 1 HCV infection was treated with HARVONI for 24 weeks. The median age was 9 years (range: 6 to 11); 59% of the subjects were male; 79% were White, 8% were Black, and 6% were Asian; 10% were Hispanic/Latino; mean body mass index was 18 kg/m2 (range: 13 to 31kg/m2); mean weight was 33 kg (range 18 to 76 kg); 59% had baseline HCV RNA levels greater than or equal to 800,000 IU/mL; 86% had genotype 1a HCV infection; 2 subjects (1 treatment-na√Įve, 1 treatment-experienced) had known compensated cirrhosis. The majority of subjects (97%) had been infected through vertical transmission.
The SVR12 rate was 99% (86/87) in subjects with genotype 1 HCV infection, and 100% (2/2) in subjects with genotype 4 HCV infection. The one genotype 1 subject treated with HARVONI for 24 weeks also achieved SVR12. The one subject (genotype 1) who did not achieve SVR12 and relapsed had been treated with HARVONI for 12 weeks.
Subjects 3 Years to <6 Years of Age: HARVONI was evaluated in 34 subjects 3 years to <6 years of age with HCV genotype 1 (N = 33) or genotype 4 (N = 1) infection. All of the subjects were treatment-na√Įve and treated with HARVONI for 12 weeks. The median age was 5 years (range: 3 to 5); 71% of the subjects were female; 79% were White, 3% were Black, and 6% were Asian; 18% were Hispanic/Latino; mean body mass index was 17 kg/m2 (range: 13 to 25 kg/m2); mean weight was 19 kg (range 11 to 34 kg); 56% had baseline HCV RNA levels greater than or equal to 800,000 IU/mL; 82% had genotype 1a HCV infection; no subjects had known cirrhosis. All subjects (100%) had been infected through vertical transmission.
The SVR12 rate was 97% (32/33) in subjects with genotype 1 HCV infection, and the one subject with genotype 4 HCV infection also achieved SVR12. One subject prematurely discontinued study treatment due to an adverse event.
16 How Supplied/storage And Handling
STORAGE AND HANDLING SECTION
Tablets
HARVONI tablets 90 mg/400 mg are orange, diamond-shaped, film-coated, debossed with "GSI" on one side and "7985" on the other side of the tablet. Each bottle contains 28 tablets (NDC 61958-1801-1), a silica gel desiccant and polyester coil, and is closed with a child-resistant closure.
HARVONI tablets, 45 mg/200 mg, are white, capsule-shaped, film-coated, debossed with "GSI" on one side and "HRV" on the other side of the tablet. Each bottle contains 28 tablets (NDC 61958-1803-1), a silica gel desiccant and polyester coil, and is closed with a child-resistant closure.
- Store below 30 ¬įC (86 ¬įF).
- Dispense only in original container.
- Do not use if seal over bottle opening is broken or missing.
STORAGE AND HANDLING SECTION
Oral Pellets
HARVONI pellets, 45 mg/200 mg, are orange pellets supplied as unit-dose packets in cartons. Each carton contains 28 packets (NDC 61958-1804-1).
HARVONI pellets, 33.75 mg/150 mg, are orange pellets supplied as unit-dose packets in cartons. Each carton contains 28 packets (NDC 61958-1805-1).
- Store below 30 ¬įC (86 ¬įF).
- Do not use if carton tamper-evident seal or packet seal is broken or damaged.
17 Patient Counseling Information
Advise the patient to read the FDA-approved patient labeling (Patient Information and Instructions for Use).
Risk of Hepatitis B Virus Reactivation in Patients Coinfected with HCV and HBV
Inform patients that HBV reactivation can occur in patients coinfected with HBV during or after treatment of HCV infection. Advise patients to tell their healthcare provider if they have a history of HBV infection [see Warnings and Precautions (5.1)].
Serious Symptomatic Bradycardia When Coadministered with Amiodarone
Advise patients to seek medical evaluation immediately for symptoms of bradycardia such as near-fainting or fainting, dizziness or lightheadedness, malaise, weakness, excessive tiredness, shortness of breath, chest pain, confusion, or memory problems [see Warnings and Precautions (5.2), Adverse Reactions (6.2), and Drug Interactions (7.2)].
Drug Interactions
Inform patients that HARVONI may interact with other drugs. Advise patients to report to their healthcare provider the use of any other prescription or nonprescription medication or herbal products including St. John's wort [see Warnings and Precautions (5.2, 5.3) and Drug Interactions (7)].
Pregnancy
Advise patients to avoid pregnancy during combination treatment with HARVONI and ribavirin and for 6 months after completion of treatment. Inform patients to notify their healthcare provider immediately in the event of a pregnancy [see Use in Specific Populations (8.1)].
Hepatitis C Virus Transmission
Inform patients that the effect of treatment of hepatitis C infection on transmission is not known, and that appropriate precautions to prevent transmission of the hepatitis C virus during treatment or in the event of treatment failure should be taken.
Administration
Advise patients to take HARVONI every day at the regularly scheduled time with or without food. Inform patients that it is important not to miss or skip doses and to take HARVONI for the duration that is recommended by the physician.
For HARVONI oral pellets, advise patients or caregivers to read and follow the Instructions for Use for preparing the correct dose.
Manufactured and distributed by: Gilead Sciences, Inc. Foster City, CA 94404
HARVONI, ATRIPLA, COMPLERA, TRUVADA and VIREAD are trademarks of Gilead Sciences, Inc., or its related companies. All other trademarks referenced herein are the property of their respective owners.
© 2020 Gilead Sciences, Inc. All rights reserved. 205834-GS-011
Spl Patient Package Insert Section
This Patient Information has been approved by the U.S. Food and Drug Administration Revised: 03/2020¬†¬†¬†¬† Patient Information HARVONI¬ģ (har-VOE-nee) (ledipasvir and sofosbuvir) tablets HARVONI¬ģ (har-VOE-nee) (ledipasvir and sofosbuvir) oral pellets Important: If you take HARVONI with ribavirin, you should also read the Medication Guide for ribavirin. What is the most important information I should know about HARVONI? HARVONI can cause serious side effects, including, Hepatitis B virus reactivation: Before starting treatment with HARVONI, your healthcare provider will do blood tests to check for hepatitis B virus infection. If you have ever had hepatitis B virus infection, the hepatitis B virus could become active again during or after treatment of hepatitis C virus with HARVONI. Hepatitis B virus becoming active again (called reactivation) may cause serious liver problems including liver failure and death. Your healthcare provider will monitor you if you are at risk for hepatitis B virus reactivation during treatment and after you stop taking HARVONI. For more information about side effects, see the section "What are the possible side effects of HARVONI?" What is HARVONI? HARVONI is a prescription medicine used to treat adults and children 3 years of age and older with chronic (lasting a long time) hepatitis C virus (HCV):
- genotype 1, 4, 5, or 6 infection without cirrhosis or with compensated cirrhosis
- genotype 1 infection with advanced cirrhosis (decompensated) in combination with ribavirin
- genotype 1 or 4 infection without cirrhosis or with compensated cirrhosis who have had a liver transplant, in combination with ribavirin
It is not known if HARVONI is safe and effective in children with HCV under 3 years of age. Before taking HARVONI, tell your healthcare provider about all of your medical conditions, including if you:
- have ever had hepatitis B virus infection
- have liver problems other than hepatitis C infection
- have had a liver transplant
- have kidney problems or you are on dialysis
- have HIV infection
- are pregnant or plan to become pregnant. It is not known if HARVONI will harm your unborn baby.
- Males and females who take HARVONI in combination with ribavirin should also read the ribavirin Medication Guide for important pregnancy, contraception, and infertility information.
- are breastfeeding or plan to breastfeed. It is not known if HARVONI passes into your breast milk.
- Talk to your healthcare provider about the best way to feed your baby during treatment with HARVONI.
Tell your healthcare provider about all of the medicines you take, including prescription and over-the-counter medicines, vitamins, and herbal supplements. HARVONI and other medicines may affect each other. This can cause you to have too much or not enough HARVONI or other medicines in your body. This may affect the way HARVONI or your other medicines work, or may cause side effects. Keep a ul of your medicines to show your healthcare provider and pharmacist.
- You can ask your healthcare provider or pharmacist for a ul of medicines that interact with HARVONI.
Do not start taking a new medicine without telling your healthcare provider. Your healthcare provider can tell you if it is safe to take HARVONI with other medicines. How should I take HARVONI?
- Take HARVONI exactly as your healthcare provider tells you to take it. Do not change your dose unless your healthcare provider tells you to.
- Do not stop taking HARVONI without first talking with your healthcare provider.
- Take HARVONI tablets or oral pellets by mouth, with or without food.
- It is important that you do not miss or skip doses of HARVONI during treatment.
- For adults the usual dose of HARVONI is one 90/400 mg tablet each day.
- For children 3 years of age and older your healthcare provider will prescribe the right dose of HARVONI tablets or oral pellets based on your child's body weight.
- Tell your healthcare provider if your child has problems with swallowing tablets.
- If your healthcare provider prescribes HARVONI oral pellets for your child, see "How should I give HARVONI oral pellets to my child."
- Do not miss a dose of HARVONI. Missing a dose lowers the amount of medicine in your blood. Refill your HARVONI prescription before you run out of medicine.
If you take too much HARVONI, call your healthcare provider or go to the nearest hospital emergency room right away. How should I give HARVONI oral pellets to my child? See the detailed Instructions for Use for information about how to give or take a dose of HARVONI oral pellets.
- Administer HARVONI oral pellets exactly as instructed by your healthcare provider.
- Do not open the packet until ready to use.
- Hold the HARVONI pellets packet with the cut line on top.
- Shake the HARVONI pellets packet gently to settle the pellets.
- Tear or cut the HARVONI packet along the cut line.
- HARVONI oral pellets can be taken right in the mouth without chewing, or with food.
- If HARVONI pellets are taken with food, sprinkle the pellets on one or more spoonfuls of non-acidic soft food at or below room temperature. Examples of non-acidic foods include pudding, chocolate syrup, mashed potato, and ice cream. Take HARVONI pellets within 30 minutes of gently mixing with food and swallow the entire contents without chewing to avoid a bitter taste.
- Do not store any leftover HARVONI mixture (oral pellets mixed with food) for use at a later time. Throw away any unused portion.
What are the possible side effects of HARVONI? HARVONI can cause serious side effects, including:
- Hepatitis B virus reactivation. See "What is the most important information I should know about HARVONI?"
- Slow heart rate (bradycardia). HARVONI treatment may result in slowing of the heart rate along with other symptoms when taken with amiodarone (Cordarone¬ģ, Nexterone¬ģ, Pacerone¬ģ), a medicine used to treat certain heart problems. In some cases bradycardia has led to death or the need for a heart pacemaker when amiodarone is taken with HARVONI. Get medical help right away if you take amiodarone with HARVONI and get any of the following symptoms:
- fainting or near-fainting
- dizziness or lightheadedness
- not feeling well
- weakness
- extreme tiredness
- shortness of breath
- chest pains
- confusion
- memory problems
The most common side effects of HARVONI include:
- tiredness
- headache
- weakness
These are not all the possible side effects of HARVONI. For more information, ask your healthcare provider or pharmacist. Call your doctor for medical advice about side effects. You may report side effects to FDA at 1-800-FDA-1088. How should I store HARVONI?
- Store HARVONI tablets or pellets below 86¬įF (30¬įC).
- Keep HARVONI tablets in the original container.
- Do not use HARVONI tablets if the seal over the bottle opening is broken or missing.
- Do not use HARVONI pellets if the carton tamper-evident seal, or the pellets packet seal, is broken or damaged.
Keep HARVONI and all medicines out of the reach of children. General information about the safe and effective use of HARVONI Medicines are sometimes prescribed for purposes other than those uled in a Patient Information leaflet. Do not use HARVONI for a condition for which it was not prescribed. Do not give HARVONI to other people, even if they have the same symptoms you have. It may harm them. You can ask your healthcare provider or pharmacist for information about HARVONI that is written for health professionals. What are the ingredients in HARVONI? Active ingredients: ledipasvir and sofosbuvir Inactive ingredients, Tablets 90/400 mg: colloidal silicon dioxide, copovidone, croscarmellose sodium, lactose monohydrate, magnesium stearate, and microcrystalline cellulose. The tablet film-coat contains: FD&C yellow #6/sunset yellow FCF aluminum lake, polyethylene glycol, polyvinyl alcohol, talc, and titanium dioxide. Inactive ingredients, Tablets 45/200 mg: colloidal silicon dioxide, copovidone, croscarmellose sodium, lactose monohydrate, magnesium stearate, and microcrystalline cellulose. The tablet film-coat contains: polyethylene glycol, polyvinyl alcohol partially hydrolyzed, talc, and titanium dioxide. Inactive ingredients, Oral Pellets: amino-methacrylate copolymer, colloidal silicon dioxide, copovidone, croscarmellose sodium, hypromellose, iron oxide red, iron oxide yellow, lactose monohydrate, magnesium stearate, microcrystalline cellulose, polyethylene glycol, talc, and titanium dioxide. Manufactured and distributed by: Gilead Sciences, Inc., Foster City, CA 94404 For more information, call 1-800-445-3235 or go to www.HARVONI.com. HARVONI is a trademark of Gilead Sciences, Inc. All other trademarks referenced herein are the property of their respective owners. ©2020 Gilead Sciences, Inc. All rights reserved. 205834-GS-011
Instructions For Use Harvoni (har-voe-nee) (ledipasvir And Sofosbuvir) Pellets, For Oral Use
Read the Patient Information that comes with HARVONI oral pellets for important information about HARVONI.
This Instructions for Use contains information on how to take HARVONI oral pellets. Be sure you understand and follow the instructions. If you have any questions, ask your healthcare provider or pharmacist.
Important Information You Need to Know Before Taking HARVONI oral pellets
- For oral use only (take by mouth with or without food).
- Do not open the HARVONI oral pellet packet(s) until ready to use.
- HARVONI oral pellets are orange pellets supplied as single-use packets in cartons. Each carton contains 28 packets.
- Do not use HARVONI oral pellets if the carton tamper-evident seal, or the pellets packet seal, is broken or damaged.
Preparing a dose of HARVONI oral pellets to be taken with food:
Before you prepare a dose of HARVONI oral pellets to be taken with food, gather the following supplies:
- Daily HARVONI oral pellet packet(s), as prescribed by your healthcare provider
- One or more spoonfuls of non-acidic soft food such as pudding, chocolate syrup, mashed potato, or ice cream
- Bowl
- Spoon
- Scissors (optional)
Step 1: Add one or more spoonfuls of non-acidic soft food to the bowl first.
Step 2: Hold the HARVONI oral pellets packet with the cut line on top (see Figure A ). Step 3: Shake the packet gently to settle the pellets to the bottom of the packet (see Figure B ). 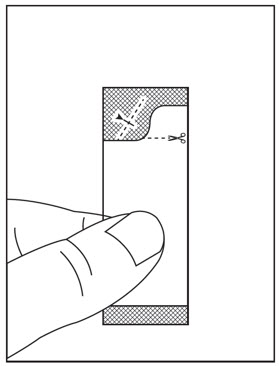
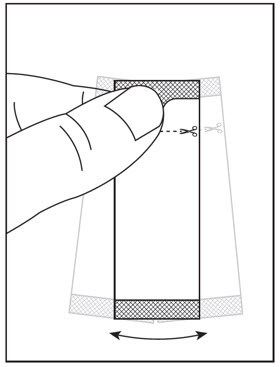
Figure A Figure B
Step 4: Cut the packet along the cut line with scissors (see Figure C ), or fold the packet back at the tear line (see Figure D ) and tear open (see Figure E ).
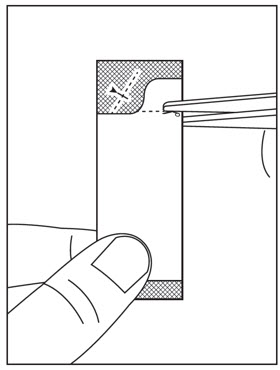

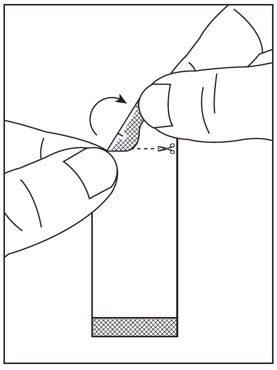
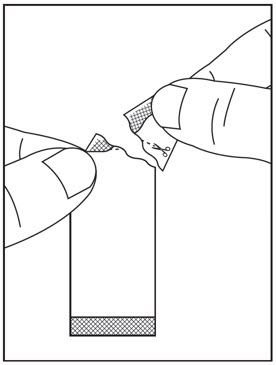
Figure C Figure D Figure E
Step 5: Carefully pour the entire contents of the prescribed number of HARVONI oral pellet packet(s) onto the food in the bowl and gently mix with a spoon (see Figure F ). Make sure that no HARVONI oral pellets remain in the packet(s).
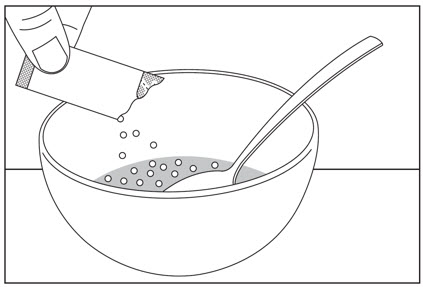
Figure F
Step 6: Take the HARVONI oral pellets and food mixture within 30 minutes without chewing to avoid a bitter taste. Ensure all of the HARVONI oral pellets are taken.
Preparing a dose of HARVONI oral pellets to be taken without food:
Before you prepare a dose of HARVONI oral pellets to be taken without food, gather the following supplies:
- Daily HARVONI oral pellet packet(s), as prescribed by your healthcare provider
- Scissors (optional)
- Water (optional)
Step 1: Hold the HARVONI oral pellets packet with the cut line on top (see Figure G ). Step 2: Shake the packet gently to settle the pellets to the bottom of the packet (see Figure H ). 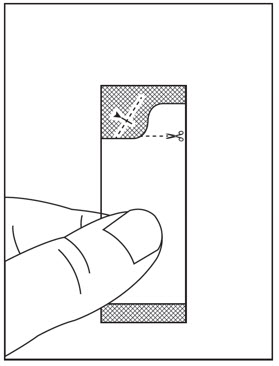
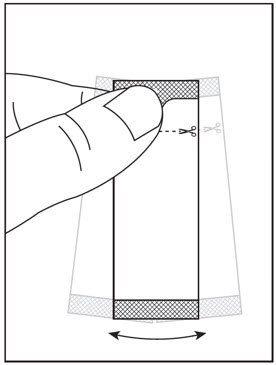
Figure G Figure H
Step 3: Cut the packet along the cut line with scissors (see Figure I ), or fold the packet back at the tear line (see Figure J ) and tear open (see Figure K ).
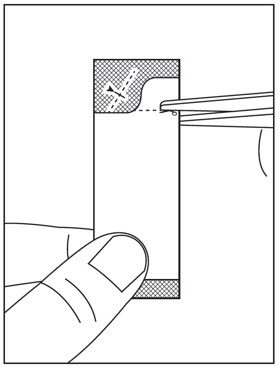

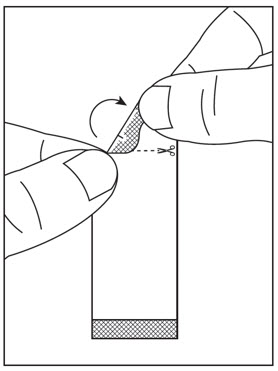
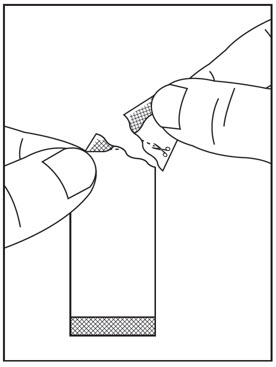
Figure I Figure J Figure K
Step 4: Pour the entire contents of the HARVONI oral pellets packet directly in the mouth and swallow without chewing to avoid a bitter taste (see Figure L ). Water may be taken after swallowing the pellets, if needed. Make sure that no HARVONI oral pellets remain in the packet. If your healthcare provider prescribed more than one HARVONI oral pellets packet, repeat Steps 1 through 4.
Figure L
Storing HARVONI oral pellets
- Store HARVONI pellets below 86¬įF (30¬įC).
- Keep HARVONI oral pellets and all medicines out of the reach of children.
Disposing of HARVONI oral pellets
- Throw away any unused portion. Do not store and reuse any leftover HARVONI mixture (pellets mixed with food).
For more information, call 1-800-445-3235 or go to www.HARVONI.com.
Manufactured for and distributed by: Gilead Sciences, Inc., Foster City, CA 94404HARVONI is a trademark of Gilead Sciences, Inc., or its related companies.
© 2020 Gilead Sciences, Inc. All rights reserved.205834-GS-011
This Instructions for Use has been approved by the U.S. Food and Drug Administration.Issued: March 2020
Principal Display Panel - 90 Mg/400 Mg Tablet Bottle Label
NDC 61958-1801-128 tablets
Harvoni¬ģ (ledipasvir, sofosbuvir)tablets, 90 mg/400 mg
Take 1 tablet once daily
Note to pharmacist:Do not cover ALERT box with pharmacy label.
ALERT: Find out about medicines thatshould NOT be taken with Harvoni
Principal Display Panel - 45 Mg/200 Mg Tablet Bottle Label
NDC 61958-1803-128 tablets
Harvoni¬ģ (ledipasvir, sofosbuvir)tablets
45 mg/200 mg
Note to pharmacist:Do not cover ALERT box with pharmacy label.
ALERT: Find out about medicines thatshould NOT be taken with Harvoni
Principal Display Panel - 33.75 Mg/150 Mg Pellet Packet Carton Label
NDC 61958-1805-128 packets
Harvoni¬ģ (ledipasvir/sofosbuvir) oral pellets
33.75 mg/150 mg per packet
Rx only
Note to pharmacist: Do not cover ALERT box with pharmacy label.
ALERT: Find out about medicines that should NOT be taken with Harvoni
GILEAD
Principal Display Panel - 45 Mg/200 Mg Pellet Packet Carton Label
NDC 61958-1804-128 packets
Harvoni¬ģ (ledipasvir/sofosbuvir) oral pellets
45 mg/200 mg per packet
Rx only
Note to pharmacist: Do not cover ALERT box with pharmacy label.
ALERT: Find out about medicines that should NOT be taken with Harvoni
GILEAD
DISCLAIMER:
"This tool does not provide medical advice, and is for informational and educational purposes only, and is not a substitute for professional medical advice, treatment or diagnosis. Call your doctor to receive medical advice. If you think you may have a medical emergency, please dial 911."
"Do not rely on openFDA to make decisions regarding medical care. While we make every effort to ensure that data is accurate, you should assume all results are unvalidated. We may limit or otherwise restrict your access to the API in line with our Terms of Service."
"This product uses publicly available data from the U.S. National Library of Medicine (NLM), National Institutes of Health, Department of Health and Human Services; NLM is not responsible for the product and does not endorse or recommend this or any other product."
PillSync may earn a commission via links on our site
