Metaxalone (metaxalone 800 mg) Dailymed
Generic: metaxalone is used for the treatment of Anemia, Hemolytic Liver Diseases Muscle Cramp Muscle Rigidity Muscle Spasticity Myositis Pain Spasm Renal Insufficiency
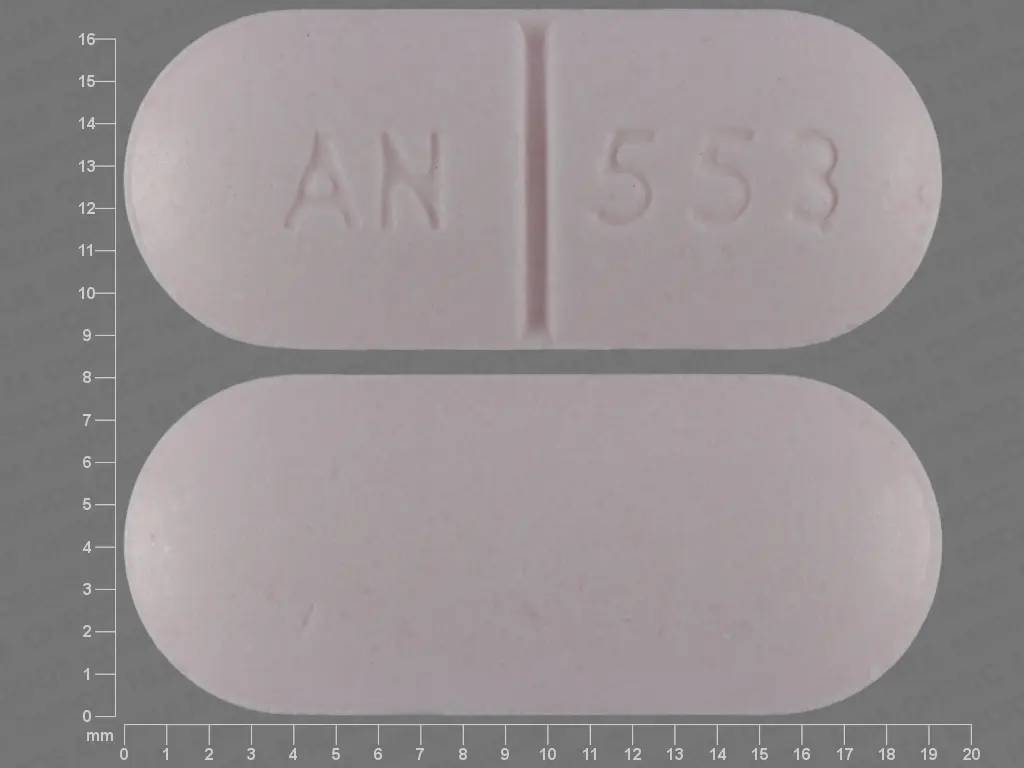
IMPRINT: AN 553
SHAPE: oval
COLOR: pink SCORE: 2
All Imprints
metaxalone 800 mg oral tablet - an 553 capsule pink
metaxalone 800 mg - an 553 capsule pink

Go PRO for all pill images
Recent Major Changes Section
Dosage and Administration (2 )                             06/2024
1 Indications And Usage
Metaxalone tablets are indicated as an adjunct to rest, physical therapy, and other measures for the relief of discomfort associated with acute, painful musculoskeletal conditions in adults and pediatric patients 13 years of age and older.
Metaxalone is a muscle relaxant indicated as an adjunct to rest, physical therapy, and other measures for the relief of discomforts associated with acute, painful musculoskeletal conditions in adults and pediatric patients 13 years of age and older. (1 )
2 Dosage And Administration
The recommended dosage of metaxalone  in adults and pediatric patients 13 years of age and older is 800 mg orally three to four times a day [see Use in Specific Populations (8)].
Metaxalone tablets 800 mg are not substitutable on a mg to mg basis with metaxalone tablets, 640 mg [see Clinical Pharmacology (12.3)]. When it is appropriate to switch:
Switch only in patients who have been taking metaxalone tablets, 640 mg on an empty stomach. Stop metaxalone tablets, 640 mg three times a day and start metaxalone tablets 800 mg three times a day on an empty stomach, OR stop metaxalone tablets 640 mg four times a day and start metaxalone tablets 800 mg four times a day on an empty stomach.
Do not switch from metaxalone tablets, 640 mg to metaxalone tablets 800 mg  when the patient is taking food during administration.
- Recommended dosage of metaxalone tablets in adults and pediatric patients 13 years of age and older is 800 mg orally three to four times a day. (
2 )- Metaxalone tablets 800 mg are not substitutable on a mg to mg basis with metaxalone tablets, 640 mg. When it is appropriate to switch, see the Full Prescribing Information on switching instructions. (
2 )
3 Dosage Forms And Strengths
Tablets: 800 mg light pink to pink, capsule shaped, scored uncoated tablet with debossing ‚ÄėAN‚Äô on the left side of the scoring and ‚Äė553‚Äô on the right side of the scoring. Other side of the tablet is plain.
Tablets: 800 mg light pink to pink, capsule shaped, scored uncoated tablet with debossing ‚ÄėAN‚Äô on the left side of the scoring and ‚Äė553‚Äô on the right side of the scoring. Other side of the tablet is plain. (3 )
4 Contraindications
Metaxalone  is contraindicated in patients with:
- Known hypersensitivity to any component of metaxalone.
- Known tendency to drug induced, hemolytic, or other anemias.
- Severe renal or hepatic impairment.
- Known hypersensitivity to any components of this product. (
4 )- Known tendency to drug induced, hemolytic, or other anemias. (
4 )- Severe renal or hepatic impairment. (
4 )
5 Warnings And Precautions
- Serotonin Syndrome: Cases of serotonin syndrome, a potentially life-threatening condition, have been reported during concomitant use of metaxalone (within the recommended dosage range) and other serotonergic drugs and with the use of metaxalone as the only serotonergic drug taken at a dosage higher than the recommended dosage. If concomitant use is warranted, carefully observe the patient, particularly during treatment initiation and dosage increases. Discontinue metaxalone if serotonin syndrome is suspected or it occurs. (
5.1 , 7.1 )- Central Nervous System (CNS) Depression: Metaxalone may impair mental and/or physical abilities required for the performance of hazardous tasks, such as operating machinery or driving a motor vehicle, especially when used with other CNS depressants including alcohol. Follow patients closely for signs and symptoms of respiratory depression and sedation. If concomitant use is warranted, closely monitor for signs of respiratory depression and sedation, particularly during treatment initiation and dosage increases. (
5.2 , 7.2 )5.1Serotonin Syndrome
Cases of serotonin syndrome, a potentially life-threatening condition, have been reported during concomitant use of metaxalone (within the recommended dosage range) and other serotonergic drugs [see Drug Interactions (7)] and with the use of metaxalone as the only serotonergic drug taken at a dosage higher than the recommended dosage [see Overdosage (10)].
Serotonin syndrome symptoms may include mental status changes (e.g., agitation, hallucinations, coma), autonomic instability (e.g., tachycardia, labile blood pressure, hyperthermia), neuromuscular aberrations (e.g., hyperreflexia, incoordination, rigidity), and/or gastrointestinal symptoms (e.g., nausea, vomiting, diarrhea). The onset of symptoms generally occurs within several hours to a few days after initiation of a serotonergic drug, but may occur later than that.
If concomitant use of metaxalone and another serotoneric drug is warranted, reassess the patient, particularly during treatment initiation and dosage increases. Discontinue metaxalone if serotonin syndrome is suspected or it occurs.
5.2Central Nervous System Depression
Because of its central nervous system (CNS) depressant effects, metaxalone may impair mental and/or physical abilities required for performance of hazardous tasks, such as operating machinery or driving a motor vehicle, especially when used with other CNS depressants including alcohol. Geriatric patients may be especially susceptible to CNS depression associated with metaxalone use. When used concomitantly, the sedative effects of metaxalone and other CNS depressants (e.g., alcohol, benzodiazepines, opioids, tricyclic antidepressants) may be additive [see Drug Interactions (7)].
Follow metaxalone-treated patients closely for signs and symptoms of respiratory depression and sedation. If concomitant use of metaxalone and another CNS depressant is warranted, closely monitor for signs of respiratory depression and sedation, particularly during treatment initiation and dosage increases.
6 Adverse Reactions
The following adverse reactions associated with the use of metaxalone were identified in clinical studies or post-marketing reports. Because some of these reactions were reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure. The most frequent reactions to metaxalone were:
- CNS: drowsiness, dizziness, headache, and nervousness or "irritability".
- Digestive: nausea, vomiting, gastrointestinal upset.
Other adverse reactions were:
- CNS: cases of serotonin syndrome have been reported during concomitant use of metaxalone (within the recommended dosage range) and other serotonergic drugs and with the use of metaxalone as the only serotonergic drug at a dosage higher than the recommended dosage [see Warnings and Precautions (5.1), Drug Interactions (7.1) and  Overdosage (10)].
- Hematologic: leukopenia; hemolytic anemia;
- Hepatobiliary: jaundice;
- Immune System: anaphylaxis, hypersensitivity reaction, rash with or without pruritus.
Most common adverse reactions (incidence >5%) are nausea and vomiting. (6 )
To report SUSPECTED ADVERSE REACTIONS, contact Amneal Pharmaceuticals at 1-877-835-5472 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
7 Drug Interactions
7.1 Serotonergic Drugs
If concomitant use of metaxalone and another serotoneric drug is warranted, carefully observe the patient, particularly during treatment initiation and dosage modification. Discontinue metaxalone if serotonin syndrome is suspected or if it occurs.
Serotonin syndrome has resulted from concomitant use of metaxalone (within the recommended dosage range) with other serotonergic drugs [see Warnings and Precautions (5.1) and  Adverse Reactions (6)].
Serotonergic drugs include selective serotonin reuptake inhibitors (SSRIs), serotonin and norepinephrine reuptake inhibitors (SNRIs), tricyclic antidepressants (TCAs), triptans, 5-HT3 receptor antagonists, opioids (particularly fentanyl, meperidine, and methadone), drugs that affect the serotonergic neurotransmitter system (e.g., mirtazapine, trazodone, tramadol), and drugs that impair metabolism of serotonin (including monoamine oxidase (MAO) inhibitors, both those intended to treat psychiatric disorders and also others, such as linezolid and intravenous methylene blue).
7.2CNS Depressants
If concomitant use of metaxalone and another CNS depressant is warranted, closely monitor for signs of respiratory depression and sedation, particularly during treatment initiation and dosage increases.
Due to the additive pharmacologic effect, concomitant use of metaxalone with other CNS depressants may increase the risk of sedation and respiratory depression [see Warnings and Precautions (5.2)].
7.3Interaction of Metaxalone with Benedicts Tests
False-positive Benedict's tests, due to an unknown reducing substance, have been noted in metaxalone-treated patients. A glucose-specific test will differentiate findings.
8 Use In Specific Populations
Geriatric Use: Metaxalone-treated geriatric patients may be especially susceptible to CNS depression. (8.5 )
8.1 Pregnancy
Risk Summary
There are no available data on metaxalone use in pregnant patients to evaluate for a drug-associated risk of major birth defects, miscarriage or other adverse maternal or fetal outcomes despite decades of metaxalone use. Reproduction studies in rats have not revealed effects on the fetus due to metaxalone.
The estimated background risk of major birth defects and miscarriage for the indicated population is unknown. All pregnancies have a background risk of birth defect, loss, or other adverse outcomes. In the U.S. general population, the estimated risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
8.2 Lactation
Risk Summary
There are no data available to evaluate the presence of metaxalone or its metabolite in either human or animal milk, the effects on the breastfed infant, or the effects on milk production. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for metaxalone and any potential adverse effects on the breastfed infant from metaxalone or from the underlying maternal condition.
8.4 Pediatric Use
Metaxalone is indicated as an adjunct to rest, physical therapy, and other measures for the relief of discomforts associated with acute, painful musculoskeletal conditions in pediatric patients 13 years of age and older. The safety and effectiveness of metaxalone in pediatric patients 12 years of age or younger have not been established.
8.5 Geriatric Use
Clinical studies of metaxalone did not include sufficient numbers of patients 65 years of age and older to determine whether they respond differently from younger adult patients.
Geriatric patients may be especially susceptible to CNS depression associated with metaxalone use [see Warnings and Precautions (5.2)].
The recommended metaxalone dosage in patients 65 years of age and older is the same as in younger adult patients. Metaxalone peak plasma concentrations (Cmax) and area under the curve (AUC) were higher in patients 65 years of age and older in the fasted state; however, a clinically significant difference was not observed when metaxalone was administered in the fed state [see Clinical Pharmacology (12.3)].
8.6Hepatic Impairment
Metaxalone is contraindicated in patients with severe hepatic impairment. Metaxalone should be used with caution and additional follow-up should be considered in patients with mild to moderate hepatic impairment. The effect of hepatic impairment on metaxalone pharmacokinetics is unknown; however, metaxalone undergoes expensive hepatic metabolism [see Clinical Pharmacology (12.3)].
8.7Renal Impairment
Metaxalone is contraindicated in patients with severe renal impairment. Metaxalone should be used with caution and additional follow-up should be considered in patients with mild to moderate renal impairment. The effect of renal impairment on metaxalone pharmacokinetics is unknown; however, metaxalone undergoes renal excretion as unidentified metabolites [see Clinical Pharmacology (12.3)].
10 Overdosage
Clinical Presentation of Metaxalone Overdose
Deaths by deliberate or accidental overdose have occurred with metaxalone, particularly in combination with other CNS depressants (including alcohol). CNS manifestations may include CNS depression, agitation, hallucinations, delusions, seizures, respiratory depression, and coma. Cardiovascular effects may include tachycardia and hypertension; hypotension has also been reported. Serotonin syndrome, leading to muscle rigidity, tremor, and hyperthermia, has been reported [see Warnings and Precautions (5.1), Drug Interactions (7.1, 7.2)].
Treatment of Metaxalone Overdose
The standard of treatment is supportive care. Monitor for CNS and respiratory depression and manage airway with oxygen as needed. Gastrointestinal decontamination procedures (including emesis) should generally be avoided because aspiration may result from CNS depression and seizures. Extracorporeal elimination such as hemodialysis or plasmapheresis have no proven clinical benefit.
Consider contacting the Poison Help line (1-800-222-1222) or a medical toxicologist for additional overdose management recommendations.
11 Description
Metaxalone tablets, USP contain 800 mg of metaxalone and the following inactive ingredients: calcium carbonate, FD&C Red #40, hypromellose, lactose monohydrate, microcrystalline cellulose, povidone, silicone dioxide, sodium starch glycolate and sodium stearyl fumarate.
Metaxalone is a muscle relaxant for oral administration.
Chemically, metaxalone is 5-[(3,5- dimethylphenoxy) methyl]-2-oxazolidinone. The molecular formula is C12H15NO3, which corresponds to a molecular weight of 221.25 g/mol. The structural formula is:
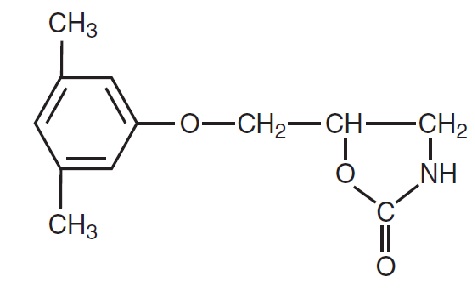
  Metaxalone, USP is a white to almost white, odorless crystalline powder freely soluble in chloroform, soluble in methanol and in 96% ethanol, but practically insoluble in ether or water.
12 Clinical Pharmacology
12.1 Mechanism of Action
Metaxalone’s mechanism of action has not been fully characterized, but may be related to its sedative properties. Metaxalone has no direct action on the contractile mechanism of striated muscle, the motor end plate, or the nerve fiber.
12.2 Pharmacodynamics
The exposure-response relationship and time course of pharmacodynamic response for the safety and effectiveness of metaxalone not been fully characterized.
12.3 Pharmacokinetics
Metaxalone pharmacokinetics were evaluated in two groups of healthy volunteers that received a single oral dose of 800 mg of metaxalone or 400 mg of metaxalone (0.5 times the approved recommended dose). Metaxalone pharmacokinetic parameters are presented below as mean (% CV) unless otherwise specified. Observed metaxalone peak plasma concentrations (Cmax) and area under the curve (AUC) are shown in Table 1. Doubling the dose of metaxalone from 400 mg (0.5 times the approved recommended dose) to 800 mg resulted in a proportional increase in metaxalone Cmax and AUC.
Table 1: Metaxalone Exposure after a Single-Dose of Metaxalone Under Fasting Conditions
Dose Cmax 2 AUC‚ąě 2
400 mg1
983 (53) ng/mL
7,479 (51) ng‚ąôh/mL
800 mg
1,816 (43) ng/mL
15,044 (46) ng‚ąôh/mL
1 0.5 times the approved recommended dose
2 Mean (% CV)
Absorption
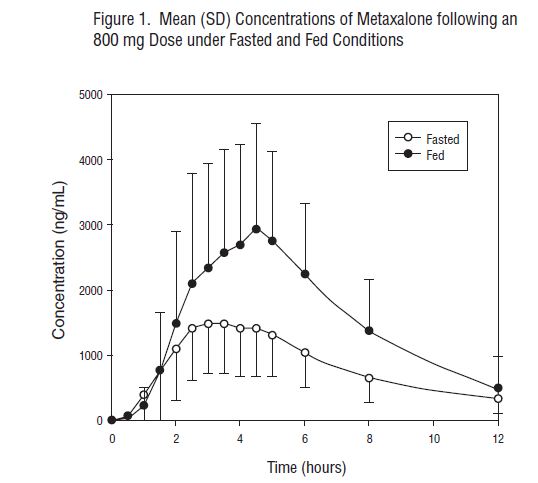
The absolute bioavailability of metaxalone is not known. Peak plasma metaxalone concentrations occurred at a mean Tmax of 3.3 hours (1.5 to 5 hours) of metaxalone under fasted conditions.
The single-dose pharmacokinetic parameters of metaxalone in two groups of healthy volunteers who received 400 mg or 800 mg of metaxalone are shown in Table 1.
Effect of Food: Peak plasma metaxalone concentrations were noted at a mean Tmax of 4.3 hours (1.5 to 12 hours) under fed conditions. The mean Tmax under fasting and fed conditions was 3.3 and 4.3 hours, respectively.
Metaxalone exposure was increased and the half-life (t1/2) was decreased following metaxalone administration with a high fat meal as shown in Table 2. The increase in metaxalone exposure coinciding with a reduction in half-life may be attributed to more complete absorption of metaxalone in the presence of a high fat meal.
 
Table 2: Relative Changes in Metaxalone Exposure, T max , and t 1/2 Following Metaxalone Administration with a High Fat Meal Compared to Fasting
Dose Cmax(ng/mL) AUC0-t(ng‚ąôh/mL) AUC0-INF(ng‚ąôh/mL) Tmax (hrs) t1/2 (hrs)
400 mg*
‚ÜĎ 78%
‚ÜĎ 24%
‚ÜĎ 15%
‚ÜĎ 30%
‚Üď 73%
800 mg
‚ÜĎ 94%
‚ÜĎ 46%
‚ÜĎ 42%
‚ÜĎ 63%
‚Üď 48%
* 0.5 times the approved recommended dose.
Distribution
Metaxalone apparent volume of distribution is approximately 800 Liters; however, plasma protein binding is unknown.
Elimination
Metaxalone mean ¬Ī SD terminal t1/2 is 9 ¬Ī 4.8 hours and apparent clearance is approximately 67 ¬Ī 34 L/h under fasted conditions.
Metabolism: Metaxalone is primarily metabolized by CYP1A2, CYP2D6, CYP2E1, and CYP3A4 and, to a lesser extent, CYP2C8, CYP2C9, and CYP2C19.
Excretion: Metaxalone is metabolized by the liver and excreted in the urine as unidentified metabolites.
Specific Populations
The effect of renal impairment and hepatic impairment on metaxalone pharmacokinetics is unknown [see Use in Specific Populations (8.6, 8.7)].
Geriatric Patients: The effects of age on the pharmacokinetics of metaxalone were determined following administration of 800 mg of metaxalone under fasted and fed conditions. Age had a significantly greater effect on metaxalone pharmacokinetics under fasted conditions than under fed conditions. Bioavailability under fasted conditions increased with age. Metaxalone bioavailability under fasted and fed conditions in the three groups of healthy volunteers of varying age is shown in Table 3.
 
Table 3: Metaxalone Pharmacokinetic Parameters under Fasted and Fed Conditions in Three Age Groups Following Oral Administration of 800 mg of Metaxalone
¬†Mean Age in Years (¬Ī SD) ¬†26 ¬Ī 9 Years Old ¬†39 ¬Ī 11 Years Old ¬†72 ¬Ī 5 Years Old ¬†Fasted vs. Fed State ¬†Fasted ¬†Fed ¬†Fasted ¬†Fed ¬†Fasted Fed¬† ¬†C max (ng/mL)1 ¬†1,816 (43) ¬†3,510 (41) ¬†2,719 (46) ¬†2,915 (55) ¬†3,168 (43) ¬†3,680 (59) ¬†T max (hours)1 ¬†3 (39) ¬†4.9 (4.8) ¬†3 (40) ¬†8.7 (91) ¬†2.6 (30) ¬†6.5 (67) ¬†AUC 0-t (ng‚ąôh/mL)1 ¬†14,531 (47) ¬†20,683 (41) ¬†19,836 (40) ¬†20,482 (37) ¬†23,797 (45) ¬†24,340 (48) ¬†AUC ‚ąě (ng‚ąôh/mL)1 ¬†15,045 (46) ¬†20,833 (41) ¬†20,490 (39) ¬†20,815 (37) ¬†24,194 (44) ¬†24,704 (47) ¬†1 Mean values (% CV)
Male and Female Patients: The exposure of metaxalone was significantly higher in females compared to males as evidenced by Cmax. (2,115 ng/mL versus 1,335 ng/mL) and AUC ‚ąě (17,884 ng‚ąôh/mL versus 10,328¬†ng‚ąôh/mL) following administration of 800 mg of metaxalone under fasted conditions. The mean half-life was 11.1 hours in females and 7.6 hours in males. The apparent volume of distribution of metaxalone was approximately 22% higher in males than in females.
Drug Interaction Studies
In Vitro Studies: Metaxalone does not inhibit CYP1A2, CYP2A6, CYP2B6, CYP2C8, CYP2C9, CYP2C19, CYP2D6, CYP2E1, and CYP3A4. Metaxalone does not induce CYP1A2, CYP2B6, and CYP3A4.
13 Nonclinical Toxicology
13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Long-term studies to evaluate the carcinogenic potential of metaxalone have not been conducted. Studies to evaluate the mutagenic potential of metaxalone have not been conducted. No effects on fertility were observed in rats administered metaxalone.
16 How Supplied/storage And Handling
Metaxalone Tablets USP, 800 mg are supplied as light pink to pink, capsule shaped, scored uncoated tablet with debossing ‚ÄėAN‚Äô on the left side of the scoring and ‚Äė553‚Äô on the right side of the scoring. Other side of the tablet is plain.
They are available as follows:
Bottles of 100:                                    NDC 65162-553-10
Bottles of 500:                                    NDC 65162-553-50
Store at 20¬į to 25¬įC (68¬į to 77¬įF); excursions permitted between 15¬į to 30¬įC (59¬į to 86¬įF) [see USP Controlled Room Temperature].
17 Patient Counseling Information
Serotonin Syndrome
Inform patients that metaxalone could cause a rare but potentially life-threatening condition called serotonin syndrome. Warn patients of the symptoms of serotonin syndrome and to seek medical attention right away if symptoms develop. Instruct patients to inform their healthcare providers if they are taking, or plan to take, serotonergic drugs [see Warnings and Precautions (5.1) and  Drugs Interactions (7.1)].
Central Nervous System Depression
Advise patients that metaxalone may impair mental and/or physical abilities required for performance of hazardous tasks, such as operating machinery or driving a motor vehicle, especially when used with alcohol and other CNS depressants [see Drug Interactions (7.2)].
 
Manufactured by:
Amneal Pharmaceuticals Pvt. Ltd.
Ahmedabad 382220, INDIA
Distributed by:
Amneal Pharmaceuticals LLC
Bridgewater, NJ 08807
Rev. 08-2024-04
Principal Display Panel
NDC 69238-1305-1
Metaxalone Tablets USP, 800 mg
Rx Only
100 Tablets
Amneal Pharmaceuticals LLC
DISCLAIMER:
"This tool does not provide medical advice, and is for informational and educational purposes only, and is not a substitute for professional medical advice, treatment or diagnosis. Call your doctor to receive medical advice. If you think you may have a medical emergency, please dial 911."
"Do not rely on openFDA to make decisions regarding medical care. While we make every effort to ensure that data is accurate, you should assume all results are unvalidated. We may limit or otherwise restrict your access to the API in line with our Terms of Service."
"This product uses publicly available data from the U.S. National Library of Medicine (NLM), National Institutes of Health, Department of Health and Human Services; NLM is not responsible for the product and does not endorse or recommend this or any other product."
PillSync may earn a commission via links on our site
